
February 23, 2026
Addressing Chronic Vacancies
In Prison Mental Health Care
- Introduction
- Overview of CDCR Prison Mental Health Care
- Current Efforts to Address Chronic Mental Health Vacancies
- Continued State Effort to Address Vacancies Is Critical
- Assessment of Additional Steps to Address Chronic Vacancies
- Recommendations
- Conclusion
Executive Summary
Prisons Have Struggled to Provide Mental Health Care and Address Chronic Mental Health Staff Vacancies. For over three decades, the California Department of Corrections and Rehabilitation (CDCR) has faced litigation for providing unconstitutional levels of prison mental health care, in part due to chronic vacancies among mental health staff. As a result, a series of federal court orders—in the case now known as Coleman v. Newsom—have directed the state to make various changes, including reducing vacancy rates below 10 percent in certain key mental health classifications. However, CDCR has struggled to meet this standard for various reasons, including the challenging working conditions at prisons and the limited pool of providers where prisons are located. In September 2025, the court—citing, in part, the ongoing failures to reduce vacancies—established a mental health Receivership “to take control of the delivery of mental health services.” This will result in a significant loss of autonomy for the state in the delivery of prison mental health care.
Continued State Effort to Address Vacancies Is Critical. Despite the Receivership, the Legislature will retain the ability to approve, reject, or modify the Receiver’s budget proposals, pass legislation mandating CDCR to take specific actions, and conduct oversight of the system. Additionally, chronic mental health vacancies likely affect mental health outcomes and addressing them will be essential to returning authority back to the state. Accordingly, it is critical for the state to continue to take action to reduce mental health vacancies.
Recommend Legislature Take Various Steps to Reduce Chronic Vacancies. To address chronic mental health staffing vacancies, we recommend the Legislature take the following the steps:
- Assess Effectiveness of Other Steps Before Considering Across‑the‑Board Pay Increases. For various reasons, including that current CDCR compensation appears to meet or exceed market rates and factors outside of compensation likely play a major role in the state’s ability to staff mental health positions, we recommend the Legislature not provide significant across‑the‑board compensation increases in the near term, though more targeted increases could be appropriate.
- Eliminate the Requirement for Licensed Out‑of‑State Providers to Get California Licenses. This would allow CDCR to benefit from recruiting from a wider pool of applicants. We also recommend directing CDCR to recruit more from out of state.
- Increase Use of CDCR Tele‑Mental Health to Maximum Court‑Approved Levels. The Coleman court allows up to half of providers to patients not in inpatient beds to provide services through tele‑mental health. Even under a proposed expansion, however, only about 30 percent of providers will be remote. Further expanding tele‑mental health could attract qualified professionals who might not otherwise want to work in a prison setting, as well as allow the state to recruit from areas where there are more providers available.
- Ask Court to Allow Tele‑Mental Health Providers to Work From Out of State. This would open up a potentially large pool of new applicants who are interested in working for CDCR but would prefer not to move from their current location.
- Require CDCR Report on the Feasibility of Concentrating Mental Health Population in Prisons That Are Easier to Staff. Concentrating the mental health population could have various benefits, such as making it easier to recruit staff located in areas with a wider pool of applicants and reducing the need for staff at locations with large vacancies. However, this could prove logistically difficult. Having a report that explores the feasibility and costs of this option would better position the state and the Legislature to know what the challenges of such an approach are.
- Direct CDCR to Align Inpatient Capacity With Actual Need. CDCR is operating hundreds more inpatient beds than the amount projected to be necessary. This increases costs and the number of positions it needs to fill unnecessarily. We recommend directing CDCR to request the Receiver to allow it to operate only the inpatient beds projected to be necessary.
Taken together, these steps will help the state better recruit and retain mental health staff, reduce the state’s reliance on expensive contracted staff, meet its constitutional requirements, lead to more effective care, and help return the mental health system to state control.
Introduction
For many years, the California Department of Corrections and Rehabilitation’s (CDCR’s) mental health system has struggled to employ an adequate number of qualified staff. As a result of this chronic deficiency and others, CDCR has faced litigation for over three decades contending that it has not provided adequate mental health care. This culminated in a federal court appointing a mental health Receiver to take direct control over the prison mental health care system. The only way the state will be able to regain full control of the system is through addressing its deficiencies, which includes hiring and retaining qualified mental health care staff. The purpose of this report is to provide an overview of CDCR’s mental health system, assess ongoing efforts to address mental health vacancies as well as additional steps that could be taken to reduce vacancies, and make recommendations aimed at bolstering the state’s ability to recruit and retain sufficient mental health staff.
Overview of CDCR Prison Mental Health Care
Prevalence of Mental Health Need in Prison
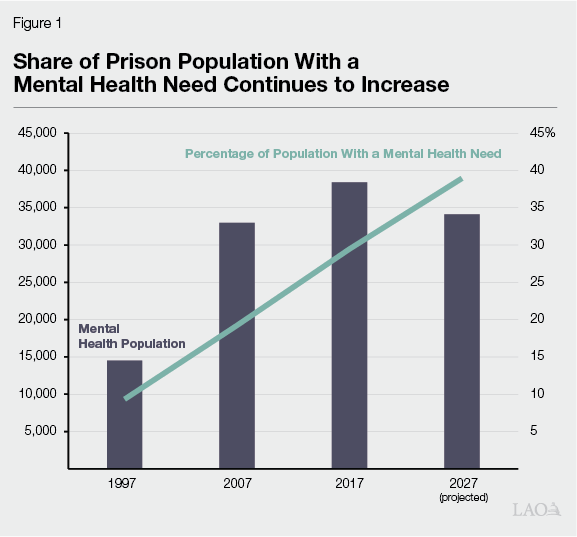
About Two Out of Five People in Prison Receive Mental Health Services. Nearly 35,000 people in prison have a diagnosed mental health need. Compared to a few decades ago, this represents significant growth. For example, Figure 1 shows that in 1997 there were about 14,500 people in prison with a mental health need which represented about 10 percent of the overall prison population. However, in more recent years, the prison mental health population has generally decreased and is projected to continue to decline. This is due to the significant reduction in the overall number of people in prison. However, the mental health population has not declined as quickly as the overall population. As a result, the share of people in prison with a mental health need has increased. Although there is no conclusive explanation for what is causing this trend, CDCR has suggested that contributing factors could include an increase in the length of prison stay for those with a mental health need or the difficulty people with mental health needs have in earning credits (which allow people to be released earlier) based on behavior. Furthermore, it is possible that CDCR’s ability to identify people who have a mental health need has improved due in part to changes mandated by the federal court in a case now known as Coleman v. Newsom, which we describe next.
Coleman Court Monitoring Prison Mental Health Care Since 1990
Federal Court Found State Provided Inadequate Prison Mental Health Care. The Coleman court case, filed in 1990 and certified as a class action lawsuit in 1991, involves allegations that the state prison system provides constitutionally inadequate mental health care for people in prison. Through this litigation, the federal court found the state to be in violation of the Eighth Amendment of the U.S. Constitution—prohibiting cruel and unusual punishment—for providing inadequate prison mental health care. Since then, the Coleman court has been involved in bringing the state into compliance with constitutional standards.
Federal Court Appointed Special Master in 1995 to Monitor State Prison Mental Health Care. To monitor the state’s efforts towards remedying the problems identified in the mental health system, the court appointed a Special Master in 1995. The Coleman court Special Master has audited and tracked CDCR’s progress in addressing issues. The Special Master has also provided recommendations to mitigate problems or identify new issues for the court, which has led to court orders that CDCR must comply with. However, under the Special Master’s monitoring, CDCR maintained direct authority over the state’s prison mental health system. As we discuss later in this report, the Special Master was recently replaced by a mental health Receiver (see the nearby box for more on Receiverships). In contrast to the Special Master, the Receiver has direct authority over day‑to‑day operations of CDCR’s mental health care system.
Receiverships Are a Court’s Last Resort to Reform Prisons and Jails
The appointment of a Receiver is a legal remedy in lawsuits seeking to reform prisons and jails that is typically used as a last resort by courts. Courts appoint a Receiver in order to place a neutral expert in control of some aspect of prison or jail operations. To establish a prison or jail Receivership, the court must make various determinations, including that there is grave and immediate harm to the plaintiffs, that the use of less extreme remedies has been exhausted, and that a Receiver is able to provide a quick remedy to the constitutional violations. Receivers are appointed and provided with various powers and authority necessary to bring prisons or jails into compliance. Receiverships last until the deficiencies have been rectified and defendants can show that they can sustain the remedies. The court has discretion on how a Receivership ends based on the circumstances that led to the establishment. Two Receiverships have been established to oversee aspects of California’s prison system. The first was established in 2006 to oversee the prison medical system. For more details on the medical Receiver please see our brief Overview and Update on the Prison Receivership. The second was established in 2025 to oversee the prison mental health system. More details on the mental health Receivership are provided later in this report.
Mental Health Classifications and Treatment
Mental Health Needs Identified in Various Ways. CDCR is responsible for identifying and providing treatment to people with mental health needs in prisons. When people enter the prison system, they are routed to prisons with reception centers where they undergo various evaluations, including mental health evaluations. After completing the reception process, people are sent to prisons that can accommodate their designated security level and identified needs. Mental health needs can be identified after the reception center process as well. For example, while at their assigned prison, people may alert staff of their mental health needs. Mental health concerns may also be flagged through referrals from healthcare staff, correctional staff, or fellow incarcerated people.
Outpatient Level of Care Offered to People With Less Acute Needs. To address mental health needs, CDCR provides a range of services throughout the prison system, including outpatient care for lower acuity cases and inpatient treatment for more severe conditions, at no direct cost to the patient. In outpatient settings, people typically live in a prison housing unit and receive regular mental health treatment but do not require 24‑hour care. This level of care is provided at most prisons and is further divided into the following categories.
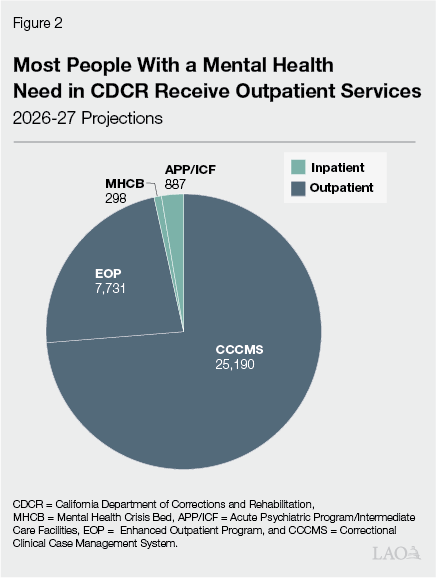
- Correctional Clinical Case Management System (CCCMS). People who require regular outpatient mental health services at the lowest levels are placed in CCCMS programming where each person is assigned a clinician and receives individual therapy at least every 90 days. As can be seen in Figure 2, CDCR projected in January 2026 there would be an average daily population of 25,200 people with a CCCMS designation in 2026‑27.
- Enhanced Outpatient Program (EOP). Those that have additional needs are placed in EOP, where they receive additional services such as weekly group therapy. CDCR seeks to place these people in separate housing units with attached medicine distribution rooms to facilitate their ability to receive psychiatric medications. CDCR projected there would be an average daily population of about 7,700 EOP patients in 2026‑27.
Inpatient Level of Care Offered to People With More Acute Needs. If a patient’s mental health condition is not stable, the patient may be referred to an inpatient level of care designed to treat higher acuity cases. Once stabilized, patients may be transitioned to outpatient services. In inpatient beds, people receive 24‑hour care and more intensive treatment beyond what is provided in outpatient programs. These beds are offered only at select locations and are divided into the following types based on the nature of the care they provide—some of which are staffed in a manner that allows them to flex between the types:
- Mental Health Crisis Beds (MHCBs). MHCBs provide short‑term housing and 24‑hour care. Due to their immediate need for treatment—often suicide prevention—people referred to MHCBs are supposed to be transferred to these beds within 24 hours. When an MHCB is unavailable at a specific prison, CDCR typically transports people to another prison with an available MHCB. Under CDCR regulations, people are not supposed to stay in MHCBs for more than ten days—but may stay longer in the same bed if it is flexed into a different inpatient bed type. Currently, CDCR is budgeted to operate 455 MHCBs—including a new 50‑bed crisis facility at the California Institution for Men in Chino. As can be seen in Figure 2, CDCR projected that an average of 298 (65 percent) of these beds would be filled on a daily basis in 2026‑27. The annual cost of operating each MHCB—whether filled or not—is around $400,000.
- Acute Psychiatric Programs (APPs). APPs provide short‑term, intensive treatment for people who show signs of a major mental illness or higher‑level symptoms of a chronic mental illness. Patients are supposed to be transferred to an APP within 72 hours of the referral, but no more than ten days after the referral and can generally stay up to 45 days. Currently, CDCR is budgeted to operate 480 APP beds, of which CDCR projected 206 (43 percent) would be filled in 2026‑27. The annual cost of operating one of these beds—whether filled or not—is $300,000.
- Intermediate Care Facilities (ICFs). ICFs provide care beyond what is provided in CDCR outpatient programs but are available for longer time periods than MHCBs or APPs. People with lower security concerns are placed in low‑custody ICFs, which are in dorms, while those with higher security concerns are placed in high‑custody ICFs, which are in cells. Currently, the state has budgeted 714 ICF beds in state prisons and 306 low‑custody ICF beds in state hospitals which CDCR can refer patients to. Of the 1,020 total ICF beds, CDCR projected 632 (62 percent) would be filled in 2026‑27. There are also 75 additional beds that can flex between ICF and APP levels of care of which 49 (65 percent) are projected to be filled in 2026‑27. Each ICF bed in a state prison costs—whether filled or not—around $246,000 annually to operate, while those in the Department of State Hospitals (DSH) cost around $393,000 annually.
Mental Health Staffing
Court Ordered Specific Staffing Levels and Current Staffing Model. A series of Coleman court orders since 2002 have dictated the levels of staffing required to operate the mental health system in the state’s prisons. Specifically, the court has ordered that CDCR must (1) establish the mental health staffing positions and budget using agreed upon ratios, (2) maintain enough mental health beds to meet the needs of the population in a timely manner, (3) maintain a 10 percent or less vacancy rate in five key mental health classifications (psychiatrists, psychologists, social workers, medical assistants, and recreational therapists), and (4) pay court‑ordered fines when vacancy rates exceed 10 percent (as we discuss in greater detail later).
Staffing Model Funds CDCR Based on Size and Composition of Mental Health Population… The annual budget for prison mental health staffing is based on a budgeting methodology that utilizes specific, court‑ordered staffing ratios that factor in the size and composition of the mental health population. Accordingly, an increase in the mental health population requires additional positions and funding, and a decline results in a reduction compared to the previous year. For example, as shown in Figure 3, if the number of EOP patients is estimated to increase by 97, the staffing ratios would indicate that one additional psychiatrist will be needed. The staffing model includes various other ratios—not listed in Figure 3—for different subpopulations.Figure 3
Size of Mental Health Population
Drives Need for Certain Positions
Ratios of Clinicians to Patients for General Outpatient Populations
|
Classification |
CCCMS |
EOP |
|
Supervising Psychologist |
1:1,200 |
1:150 |
|
Supervising Social Worker |
1:1,200 |
— |
|
Staff Psychiatrist |
1:225 |
1:97 |
|
Clinical Psychologist |
1:157 |
1:30 |
|
Social Worker |
1:157 |
1:70 |
|
Recreational Therapist |
— |
1:37 |
|
CCCMS = Correctional Clinical Case Management System and EOP = Enhanced Outpatient Program. |
||
…And the Number of Inpatient Beds. Additionally, the number of active inpatient mental health beds, which require specialized prison infrastructure, affect the level of funding and distribution of mental health staff throughout the prisons. This is because some mental health staffing positions are tied to the number of active inpatient beds as opposed to being tied directly to the mental health population. For example, CDCR receives about $400,000 and the associated positions annually for each active MHCB, irrespective of whether the bed is occupied for most of the year. In practice, CDCR can move staff around the prison as needed, especially if an inpatient bed is not occupied. As such, the number of active beds contribute to the number of positions at a given prison.
Some Mental Health Staff Work Remotely. In addition to the on‑site staff, CDCR uses tele‑mental health services to deliver mental health care. Staff who deliver tele‑mental health services use teleconferencing technology to meet with patients. These staff have the option to either commute to offices, some of which are outside of prisons, or work from home if they are able to ensure patient privacy. Generally, patients are escorted to a medical room within the prison where they communicate via audio and video with the mental health professional over a secure network.
Other Mental Health Staff Are Contractors. When CDCR lacks sufficient onsite staff to fill its positions, it hires contractors known as registry staff. Registry staff can supplement the number of mental health care staff in order to provide treatment and reduce delays in services.
Inability to Fill Mental Health Vacancies Resulted in Fines and Contributed to Appointment of a Mental Health Receiver
State Has Struggled to Comply With Court‑Ordered Staffing Levels. Since the Coleman staffing court orders were established, mental health vacancy rates have generally been above the court‑ordered 10 percent maximum and continue to remain high. Specifically, according to court records, vacancy rates in the five key classifications between April 2023 and April 2024 ranged from:
- 6 percent and 15 percent for psychiatrists.
- 35 percent and 41 percent for psychologists.
- 17 percent and 29 percent for social workers.
- 8 percent and 32 percent for medical assistants.
- 8 percent and 49 percent for recreational therapists.
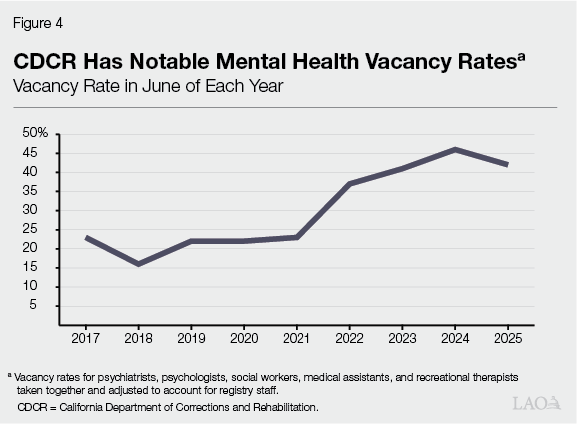
Figure 4 highlights the vacancy trends for these five classifications taken together (after accounting for registry staff) over the past nine years and shows that the vacancy rate as of June 2025 was at 43 percent. The growth in vacancy rates seen in 2022 were likely a result of a combination of factors that include staff turnover, several changes in the 2021‑22 Budget Act that added new mental health positions, and subsequent changes in the mental health population.
Court Levied Fines on State for Contempt of Court‑Ordered Staffing Levels. Due to not adequately filling mental health vacancies, in June 2024, CDCR was found to be in contempt of the court’s orders to keep vacancy rates below 10 percent. The court began levying monthly fines for vacancies in the five key classifications (psychiatrists, psychologists, clinical social workers, recreational therapists, and medical assistants). In establishing the fines, the Coleman court said that CDCR’s strategies to reduce vacancies lack urgency, have been insufficient to fill needs, and indicate that the state “is continuing to operate business as usual.” However, further collection of the fines has been paused due to the establishment of the mental health Receivership, discussed below. For further details on the fines, see the box below.
Coleman Court Found State in Contempt and Levied Fines
In June 2024, the Coleman court found the California Department of Corrections and Rehabilitation (CDCR) to be in contempt of the court’s orders and began levying fines related to mental health staffing vacancies. Beginning retroactively in April 2023, fines accrued for each of the five key classifications (psychiatrists, psychologists, clinical social workers, recreational therapists, and medical assistants) that did not achieve a 90 percent fill rate—after accounting for tele‑mental health and registry staff. As of January 2026, the court has collected $155 million in fines which were deposited into a special deposit fund called the Mental Health Staffing Deposit Fund. The court also ordered CDCR and the plaintiffs to develop a plan as to how these fines would be used. The plan developed specified that the fines would support various one‑time efforts to address vacancies, most notably by funding retention bonuses for the five classifications the state was fined for. However, additional fines have been paused due to the establishment of the mental health Receivership in September 2025. About $33 million of the fines already collected have been spent in accordance with court‑approved plans and the remainder is expected to stay in the special deposit fund to be used by the Receiver.
Court Has Established Mental Health Receivership to Address Vacancies and Improve Care More Broadly. Effective September 1, 2025, the court established a Receivership “to take control of the delivery of mental health services.” As a result, the Receiver—rather than CDCR leadership—is responsible for the day‑to‑day operations of the CDCR mental health system. Along with the establishment of the Receivership, the Coleman court has adopted the Receiver’s action plan. The plan outlines the Receiver’s strategy and efforts intended to bring the state into compliance, address court‑ordered remedies, and “achieve and retain a qualified mental health workforce.” As shown in Figure 5, the plan includes six goals—each goal accompanied by a set of actions. The Receiver estimates it will cost about $41 million annually to implement the plan and it will take between five and seven years to bring the state into compliance. The plan’s primary cost drivers are salary increases for mental health staff ($25.3 million) and additional staff—known as resource teams—at inpatient units ($6.6 million). In addition, the plan outlines that it would cost about $9 million annually to establish and operate the Office of the Receiver.
Figure 5
Receiver’s Action Plan Outlines Goals and Actions to Improve Mental Health Care
|
Goal 1 |
Improve Mental Health Care Delivery Through Culture Change and Effective Management |
|
Selected Actions |
|
|
Goal 2 |
Achieve and Retain a Qualified Mental Health Workforce |
|
Selected Actions |
|
|
Goal 3 |
Provide Adequate Care at Every Level and Treat Each Patient at the Appropriate Level of Care |
|
Selected Actions |
|
|
Goal 4 |
Fully Implement a Suicide Prevention Program |
|
Selected Actions |
|
|
Goal 5 |
Complete Development and Implementation of a Quality Assurance Program |
|
Selected Actions |
|
|
Goal 6 |
Create Mechanisms to Demonstrate Remedies |
|
Selected Actions |
|
|
CDCR = California Department of Corrections and Rehabilitation. |
|
Current Efforts to Address Chronic Mental Health Vacancies
Hiring sufficient mental health staff is not a unique challenge to CDCR. Other employers, including correctional facilities in other states, struggle to hire sufficient mental health care staff. A 2018 survey from the University of Michigan of 20 correctional facility representatives across six states found that most respondents (85 percent) agreed that they had difficulty filling open behavioral health positions and had high turnover of behavioral health staff. A wide variety of factors can make it difficult to hire and retain mental health staff at prisons, including:
- Challenging Working Conditions. Based on discussions with CDCR staff, mental health professionals may not want to work at a prison for various reasons. Staff cited concerns about safety, air conditioning and heat, lack of privacy, dilapidated or limited offices and treatment space, as well as a rigorous work schedule with few flexibilities. Finding similar concerns, the Receiver’s action plan indicates that mental health staff have an elevated fear of being assaulted in prisons.
- Limited Pool of Providers. The California Department of Health Care Access and Information in 2022 estimated for the overall California population that there is a shortage of psychiatrists and behavioral health providers in all 58 counties, with several counties experiencing severe shortages. Further, this report projected that in 2025, 16 of the state’s prisons would be in counties facing a severe shortage of mental health professionals and 11 prisons in counties facing a high shortage.
Over the last few decades, the state has taken a variety of actions aimed at addressing the chronic vacancies, including bargaining salary increases, expanding the use of registry staff, and centralizing recruitment efforts. These efforts, however, have not been sufficient to reach sustained court compliance. More recently, the state—and now the Receiver—have undertaken additional efforts to reduce vacancies. We summarize some of these recent efforts below.
State Was Pursuing Various Steps to Address Vacancies Prior to Establishment of Mental Health Receivership
In recent years, CDCR has taken various steps to maintain court‑ordered staffing levels. For example, in 2024, CDCR expanded its tele‑mental health policy by allowing social workers and psychologists (who also deliver mental health care) to work remotely in addition to psychiatrists who were previously authorized to provide such services. CDCR indicates that this has allowed them to improve recruitment and retention of these staff. Additionally, in 2025, CDCR partnered with the California Department of Human Resources (CalHR) to establish new classifications that can provide mental health services at the prisons. The classifications consist of both line and supervisory staff of marriage and family counselors as well as clinical counselors. CDCR plans to use these staff in lieu of psychiatrists and psychologists in outpatient settings, as they expect the new classifications will be easier to fill. This will allow CDCR to prioritize the psychiatrists and psychologists it is able to recruit for inpatient settings. Absent any changes from the Receiver, these various steps will continue to be implemented.
Mental Health Receiver Plans to Address Vacancies in Various Ways
The Receiver’s action plan involves various additional efforts to reduce mental health vacancies, as outlined in Figure 6, including a specific set of actions aiming to achieve and retain a qualified mental health workforce. For example, building the pipeline of providers by expanding the number of internships available at CDCR would help increase the number of providers that can work at CDCR directly—by bringing in interns—and could help CDCR’s ability to recruit them on a permanent basis. Furthermore, efforts to address concerns among mental health staff related to the safety of the prison environment could be useful. To the extent, CDCR can mitigate these concerns, people may be more open to working at a prison and staying there once employed. Moreover, increasing compensation by making the bonuses permanent may have the effect of reducing some vacancies. Finally, assessing to what degree compensation increases are necessary could be fruitful to understanding what compensation levels would induce mental health providers to work at the prisons. The other Receiver’s goals, while not directly related to staffing, depend heavily on having enough qualified mental health staff, which is why the Receiver has indicated recruitment and retention will be a key focus of the Receivership.
Figure 6
Receiver’s Action Plan to Address Mental Health Vacancies
|
Communicate to staff the high priority of filling vacancies. |
|
Implement procedures that ensure newly opened or reopened EOP, MHCB, or inpatient units have sufficient staff prior to opening. |
|
Improve onboarding process for new staff. |
|
Assess need for more staff dedicated to recruitment, hiring, and retention. |
|
Hire an internship coordinator to centralize and expand clinical internship programs. |
|
Identify strategies to reduce safety concerns among mental health staff. |
|
Maintain retention bonuses and assess whether further pay increases are needed in hard‑to‑fill locations and positions. |
|
Approve a hybrid work policy that would allow clinicians to work remotely and in person and assess whether other workplace flexibilities are possible. |
|
Decrease clinician time spent on nonclinical tasks. |
|
Complete applicant tracking system to make improvements to recruitment process. |
|
Eliminate triage plans, which have the effect of reducing treatment hours for those at the lowest levels of care. |
|
Conduct a space needs assessment at each prison and develop a plan to address those needs. |
|
EOP = Enhanced Outpatient Program and MHCB = Mental Health Crisis Beds. |
Continued State Effort to Address Vacancies Is Critical
Legislature Retains Significant Role Despite Appointment of Mental Health Receiver. The establishment of the Receivership will result in a significant loss of autonomy for the state in the delivery of prison mental health care. Despite this, the Legislature will still retain the ability to approve, reject, or modify the Receiver’s mental health system budget proposals, pass legislation mandating CDCR to take specific actions, and conduct oversight of the system. While the Receiver has the authority to ask the court to overrule such legislative actions, the Coleman court has directed the Receiver to work in a manner consistent with California state laws, regulations, and contracts. Notably, the medical Receiver appointed to oversee CDCR medical care in the Plata v. Newsom case has worked collaboratively with the state and has involved the Legislature in the decision‑making process, especially when developing the medical care budget.
Vacancies Likely Affecting Mental Health Outcomes. When an adequate number of mental health staff are not available, patients might have appointments delayed or canceled. Based on data from CDCR, 56 percent of mental health appointments were not completed as scheduled in 2024—35 percent were refused by the patient, 2 percent for custody reasons such as lockdowns, and 19 percent for other reasons such as vacancies. In addition, 47 percent of the outpatient population did not receive the necessary number of treatment hours. When patients do not receive timely treatment, it could lead to deteriorating mental health and result in self‑harm—including suicide. For example, a recent research study found that among veterans seeking mental health care in veterans’ medical centers across the country, lower mental health staffing increased the likelihood of a suicide‑related event. The results were largest among facilities that had the fewest mental health staff. While the study is not in a correctional setting, it provides a benchmark of what outcomes could result for a population with mental health needs seeking services at facilities with high vacancy rates.
To Achieve Overall Compliance, Addressing Vacancies Will Likely Be Essential. The state’s inability to fill vacancies was a strong contributor to the appointment of a mental health Receiver. As a result, addressing mental health vacancies will be essential to ending the Receivership and returning authority back to the state. Recognizing this importance, the Receiver’s action plan “places significant emphasis on building and retaining a mental health workforce because it is a foundational element to providing constitutionally adequate mental health care.” Moreover, prisons that do not struggle to fill positions appear to provide care much more effectively and have received positive feedback from the court in the past. For example, CDCR indicates that San Quentin Rehabilitation Center (SQRC) performed well in court audits prior to the appointment of the Receiver because it was more fully staffed and was able to better meet the needs of its mental health population than other prisons.
Relying on Registry Staff Is Costly to the State. To the extent the state can recruit a sufficient number of mental health staff, it could not only reduce vacancies, but also its use of costly registry staff. In December 2025, the state Auditor released a report that compared vacancy rates at three state facilities that employ mental health staff along with a comparison of hourly costs between mental health registry staff and state employees. The Auditor’s report focused on Salinas Valley State Prison (SVSP), Porterville Developmental Center, and Atascadero State Hospital. Based on the Auditor’s calculations, registry staff cost the state more at these facilities on an hourly basis than state employees, even after accounting for staff benefits, such as healthcare coverage. This difference ranges from 14 percent to 115 percent higher, depending on the position. For example, registry psychiatrists appear to cost the state about $113 (46 percent) more per hour and registry psychologists $105 (115 percent) more per hour at SVSP, after accounting for state employee benefits.
Assessment of Additional Steps to Address Chronic Vacancies
Based on discussions with CDCR providers and union representatives—as well as a review of court documents and research—we identified five different strategies the Legislature could consider as the state continues to address the chronic mental health vacancies in the prison system: (1) increasing compensation, (2) extending licensing exemptions to providers with out‑of‑state licenses, (3) expanding the use of tele‑mental health, (4) clustering patients in easier‑to‑staff prisons and (5) reducing excess inpatient capacity. In the subsequent sections, we describe and assess each option.
Increasing Compensation
Increased Compensation Is a Common Strategy to Improve Recruitment and Retention. When employers increase compensation—either in the form of higher pay or augmentations to other employer‑funded benefits (for example, higher employer contributions toward health premiums)—they typically receive more qualified applicants for a given job and people already employed are less likely to leave. Thus, it stands to reason that increasing compensation—especially if it is lagging other employers—could be one strategy to improve CDCR’s recruitment and retention of mental health staff.
Compensation Study Shows Pay for Most Mental Health Staff Leading Other Employers. To inform the collective bargaining process, CalHR conducts compensation studies to determine how state pay rates compare to the market rate for various classifications. Although the methodology for comparing the state’s total compensation has notable limitations, it is often the best information available to the state. CalHR produced the most recent compensation study of Unit 19 (Health and Social Services/Professional) in 2023, which includes three of the five key mental health classifications working at state prisons. CalHR’s study found that the state’s compensation was higher than the market for: recreational therapists (found to lead the market by 14 percent in total compensation and 11 percent above market in wages alone); clinical, counseling, and school psychologists (found to lead the market by 10 percent in total compensation and 5 percent in wages ); and healthcare social workers (found to lead the market by 14 percent in total compensation and 8 percent in wages). Since the 2023 compensation study, these classifications have also had general salary increases and pay bonuses resulting from Coleman court actions. While more recent data is not yet available, it seems plausible, based on the magnitude of the gap between state pay and other employers and the recent bonuses extended to these classifications, that the state still maintains a lead in these occupations.
Bonuses for Psychiatrists May Largely Eliminate Pay Gap With Other Employers. The most recent compensation study for Bargaining Unit 16, which represents state psychiatrists, evaluated state psychiatrist pay and found it below market (6 percent below market when comparing total compensation and 1 percent below market when comparing wages alone). The findings from the compensation study suggest that lagging wages could be a contributing factor to the high vacancy rates among psychiatrists. However, the most recent contract with Unit 16 increased state psychiatrist pay by 3 percent across all state departments. For more on the Unit 16 agreement, please see MOU Fiscal Analysis: Bargaining Unit 16 (Physicians, Dentists, and Podiatrists). Additionally, the Coleman court’s pay bonuses increased the pay by roughly 3 percent as well for those working in prisons. These two changes may largely eliminate the gap for state employees compared to other employers, though this could be eroded if other employers also increase their salaries at similar or larger rates.
Factors Outside of Compensation Likely Play a Major Role in Ability to Hire and Retain Staff. Although changes in compensation likely can affect the state’s ability to hire and retain staff, our analysis of vacancy rates at California prisons—across different classifications and between different prisons—suggests that other factors play an outsized role in vacancy rates at many prisons. First, many of the classifications with relatively high compensation rates also have high vacancy rates. For example, although the compensation study shows that in 2023 state social workers led the market, CDCR social workers had a vacancy rate of about 27 percent in 2023—higher than the statewide average. Second, despite pay being largely similar between prisons, some prisons have much lower vacancy rates—including a couple with rates that comply with Coleman court requirements. As shown in Figure 7, vacancy rates at prisons range from 6 percent to 70 percent. This suggests that factors unrelated to pay—such as challenging working conditions and a limited pool of providers available—very likely affect the state’s ability to fill mental health vacancies at most prisons.
Figure 7
Mental Health Vacancy Rates Vary by Prison
|
County |
Prison |
Mental Health Vacancy Ratea |
|
Lassen |
High Desert State Prison |
69.9% |
|
Solano |
California Medical Facility |
62.5 |
|
Monterey |
Salinas Valley State Prison |
62.4 |
|
Kern |
North Kern State Prison |
57.9 |
|
San Joaquin |
California Health Care Facility |
56.6 |
|
Kings |
California State Prison, Corcoran |
54.1 |
|
Kern |
Wasco State Prison |
53.8 |
|
Kings |
Substance Abuse Treatment Facility and State Prison |
51.4 |
|
Imperial |
Calipatria State Prison |
48.8 |
|
Amador |
Mule Creek State Prison |
48.6 |
|
Kern |
California Correctional Institution |
47.6 |
|
Los Angeles |
California State Prison, Los Angeles County |
46.4 |
|
Kern |
Kern Valley State Prison |
45.5 |
|
Del Norte |
Pelican Bay State Prison |
45.1 |
|
Fresno |
Pleasant Valley State Prison |
39.0 |
|
Sacramento |
California State Prison, Sacramento |
37.3 |
|
San Diego |
Richard J. Donovan Correctional Facility |
35.6 |
|
San Luis Obispo |
California Men’s Colony |
33.4 |
|
Kings |
Avenal State Prison |
32.8 |
|
San Bernardino |
California Institution for Men |
28.4 |
|
Monterey |
Correctional Training Facility |
27.3 |
|
Madera |
Central California Women’s Facility |
25.5 |
|
Sacramento |
Folsom State Prison |
22.1 |
|
Riverside |
California Institution for Women |
21.3 |
|
Imperial |
California State Prison, Centinela |
21.1 |
|
Riverside |
Ironwood State Prison |
21.1 |
|
Tuolumne |
Sierra Conservation Center |
19.0 |
|
Madera |
Valley State Prison |
15.3 |
|
Solano |
California State Prison, Solano |
13.3 |
|
Marin |
San Quentin Rehabilitation Center |
8.5 |
|
Riverside |
California Rehabilitation Center |
5.6 |
|
aAverage of all mental health vacancies between January 2025 and August 2025. |
||
Receiver Examining Pay Increases as Part of Action Plan. Given the importance of non‑compensation factors in determining vacancy rates, it is unclear what level of pay increase would be needed to meaningfully improve recruitment and retention for mental health positions. However, as discussed above, the Receiver will be studying potential pay increases as part of the action plan. Depending on the findings of that analysis, the Receiver may propose pay increases, which would give the Legislature an opportunity to evaluate whether they are necessary at that time.
Increasing Compensation Can Be a High‑Cost Strategy. In general, compensation increases can be a high‑cost strategy for filling vacancies. For example, the action plan estimates that it will cost $25 million ongoing to increase pay by roughly 3 percent for mental health positions at CDCR. Those salary costs would directly increase the state’s costs for benefits where the employer’s cost is determined as a percentage of pay (often referred to as “salary‑driven” benefits) like employer contributions to pension benefits. Although there might be ways to target compensation to the prisons or classifications with the greatest recruitment and retention challenges, the costs could still be substantial. Furthermore, changes in CDCR pay might have other indirect effects on mental health care programs operated by other state agencies such as DSH. Those departments may seek increases in compensation to ensure their pay remains competitive with CDCR—potentially adding still more costs to the state.
Extending Licensing Exemptions to Out‑of‑State Licensed Providers
State Licensing Policies Limit Pool of Potential Providers. Licensing restrictions limit the number of people that can work as mental health providers in California prisons. Generally, to become a mental health provider in California, a person must obtain a California license. For example, clinical social workers must obtain licensure from the California Board of Behavioral Sciences. This requires meeting the necessary education requirements, completing exams, and having a sufficient number of hours in the field. People that are licensed in other states must apply for a California license through the appropriate licensing board, meet certain requirements, and in some cases complete further education or training to become licensed in California.
State Allows Some Limited Licensing Exemptions for People Working in Prisons. Under existing law, the Board of Behavioral Sciences, which oversees licenses for clinical social workers and marriage and family therapists, as well as the Board of Psychology, which oversees licenses for psychologists, allow limited exemptions to licensing for those working in special settings, such as a correctional facility. For example, state law generally allows out‑of‑state mental health providers to work at prisons. However, those providers must obtain a California license within a set amount of time of working at CDCR and these exemptions do not apply to psychiatrists, which are licensed through the Medical Board of California.
Additional Licensing Exemptions Could Expand the Pool of Providers. CDCR could benefit from recruiting from a wider pool of applicants, particularly those from out of state that already hold licenses in their respective states. Removing the requirement that people with out‑of‑state licenses obtain a California license could help with these recruiting efforts. Notably, CDCR and CalHR would retain their current roles in identifying qualified recruits and providing the necessary training and supervision to ensure people are performing their duties adequately. This would help to ensure that the quality of care is maintained.
Expanding Use of Tele‑Mental Health
Expanding Tele‑Mental Health Could Help Address Prison Environment Concerns. Tele‑mental health could be a particularly useful tool for providing services at hard‑to‑staff prisons. Indeed, CDCR has stated that tele‑mental health positions have been easier to hire since it started expanding tele‑mental health. Because providers delivering tele‑mental health services do not have to be physically present at a prison, this means that some of the concerns that accompany being on‑site are addressed. For example, people working remotely likely do not face the same level of safety concerns that workers on site may experience when walking through a prison and interacting with various incarcerated people. Additionally, they can have more privacy and do not need to work in dilapidated facilities that may lack air conditioning. Finally, offering more tele‑mental health positions could allow CDCR to recruit staff from areas of the state where there is a larger pool of providers available.
State Has Room to Utilize More Tele‑Mental Health. Despite these potential benefits, CDCR does not appear to be taking full advantage of this option. While CDCR is not allowed to use tele‑mental health services in inpatient settings, the Coleman court allows up to 50 percent of outpatient providers—those working with the CCCMS or EOP populations—to be remote. As of September 2025, only 23 percent of outpatient providers are remote. Notably, the Governor’s proposed 2026‑27 budget requests $8.9 million General Fund growing to $12.8 million by 2028‑29 and ongoing to expand tele‑mental health services. Under the proposal, 100 existing on‑site clinicians would be redirected to tele‑mental health. The additional resources would fund supervisory and support staff (such as the on‑site medical assistants that help clinicians during tele‑mental health appointments) and equipment. While this proposed expansion is laudable, it would increase the rate of remote providers roughly to 30 percent—still 20 percentage points below the court allowed limit. (For more on this proposal, including some concerns we have with the amount of resources requested, please see the “Tele‑Mental Health” section in our brief The 2026‑27 Budget: California Department of Corrections and Rehabilitation.)
Allowing Tele‑Mental Health Staff to Work Outside of California Could Attract More Providers. Currently, the Coleman court requires tele‑mental health staff to provide services from California. This requirement from the court unnecessarily limits the pool of potential applicants to people living or willing to relocate to California. If the state—working with the court—allowed tele‑mental health providers to work outside of California, it could likely attract a much larger pool of qualified professionals. Moreover, California often pays mental health professionals more than other states. For example, CDCR psychologists, according to the state Auditor, earn between $56 and $85 per hour—well above the average hourly rate paid in other states. According to 2023 data from the Bureau of Labor Statistics, California is the highest paying state for psychologists with the average hourly wage at $64 per hour, whereas psychologists nationwide earned a median of $53 per hour (21 percent less). If people in other states were allowed to provide tele‑mental health services in California prisons, the state might be able to attract qualified candidates living in lower‑cost‑of‑living areas with higher pay, while still allowing them to maintain their residency in other states. This would be further facilitated if these candidates were also not required to obtain California licenses, as discussed previously.
Clustering in Easier‑to‑Staff Prisons
High Vacancy Rates Can Be a Self‑Perpetuating Cycle. High vacancy rates themselves might make working at a prison undesirable. This is because existing mental health staff typically have increased workload when there are many vacancies. They may also lack the peer and supervisory support to maintain a positive morale. This can mean that vacancy rates that are already elevated due to the environment inside prisons become exacerbated, making recruitment and retention especially difficult. As discussed earlier, vacancy rates vary widely by prison. This suggests that certain prisons are more challenging to staff than others. By continuing to place people with mental health needs at hard‑to‑staff prisons, CDCR must recruit mental health staff where few are available or willing to work, contributing to chronic vacancies.
Placement of Mental Health Patients in Easier‑to‑Staff Prisons Could Help Reduce Vacancies. If CDCR moves patients from hard‑to‑staff prisons to easier‑to‑staff prisons, it would help address the vacancy problem in two ways. First, the positions added to the easier‑to‑staff prisons would be more likely to be filled. Second, reducing the number of patients and vacant positions at the hard‑to‑staff facilities would mean the mental health staff remaining at those prisons would not be stretched as thin, which could improve retention and, possibly, recruitment at those prisons. The benefits of operating a prison in easier‑to‑recruit areas can be seen at SQRC in Marin. SQRC has had more success in hiring mental health staff than most other prisons, resulting in fewer vacancies. In July and August 2025, SQRC’s vacancy rate was 0 percent—well under the court‑ordered 10 percent vacancy rate. During a site visit in July 2025, SQRC staff noted that retention was high at the prison, and that new applicants have had to be placed on the waitlist because of how well staffed the prison is. Staff at the prison have indicated that this improves the prison’s ability to deliver care, increases morale, and makes the prison a more desirable place to work.
Eliminating Excess Inpatient Bed Capacity
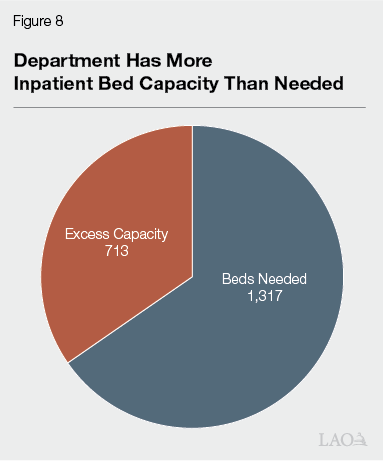
Excess Inpatient Capacity Means CDCR Trying to Fill More Vacancies and Spending More Than Necessary. As discussed in the “Inpatient Mental Health Beds” section in our brief The 2025‑26 Budget: California Department of Corrections and Rehabilitation and shown in Figure 8, CDCR is operating 713 inpatient beds in excess of the amount projected to be necessary. Operating excess inpatient beds at this scale costs the state over $200 million each year and requires that the state maintain many mental health positions more than the projections show are necessary. Moreover, maintaining these unnecessary beds means that the state is required to staff them, regardless of whether people are treated in them, artificially inflating the vacancy rate. This makes it more difficult for the state to comply with the Coleman court’s order to reduce mental health vacancies.
CDCR Taking Steps to Address Excess Capacity but Could Go Further. In court filings, CDCR indicated to the Coleman court that it planned to deactivate 249 inpatient beds because “from September 2024 to present, between 40 percent and 48 percent of inpatient beds have been empty and unused.” CDCR informed the court that closing such beds would still provide a sufficient buffer to accommodate fluctuations in the inpatient mental health population in the near term. These efforts to deactivate 249 inpatients beds are laudable. At the time of this publication, the mental health Receiver had approved CDCR’s request to close 100 excess inpatient beds and was deliberating on whether to deactivate additional excess inpatient beds. However, based on the most recent projections, even if the Receiver allowed all 249 beds to be closed, it would still leave 464 excess inpatient beds in 2026‑27. Therefore, it seems reasonable that the state could go further in deactivating additional excess beds. This option could result in about $200 million in less spending to support the 713 beds if these beds were eliminated. In addition, this could reduce the mental health vacancy rate. For example, in court documents, CDCR estimated that the staff fill rate for ICF and APP beds in June would have been 98 percent for psychiatrists (instead of 81 percent), 73 percent for psychologists (instead of 52 percent), 105 percent for social workers (instead of 82 percent), and 127 percent for recreational therapists (instead of 101 percent) had all 249 inpatient beds been deactivated that month.
Recommendations
CDCR’s actions and the mental health Receiver’s proposed actions include promising efforts to address vacancies. For example, the creation of new classifications is a promising step as it would allow treatment to be provided by potentially easier‑to‑recruit, lower‑cost positions. In addition, the Receiver’s plan would also increase the pool of people that can provide services to the mental health population by expanding clinical internship slots across the prisons. Not only will interns perform work while part of the program, but it is also possible that they will become employed permanently by CDCR. However, the plans put forward by CDCR and the Receiver could go further in addressing the barriers to filling vacancies. Below, we provide recommendations for the Legislature—some of which need coordination with the Receiver and the Coleman court to implement—as it seeks to address the chronic mental health vacancies facing CDCR.
Assess Effectiveness of Other Steps Before Considering Across‑the‑Board Pay Increases. We found that (1) most mental health classifications appear to be relatively well paid compared to the broader market even before recent bonuses, (2) other non‑compensation factors appear to influence vacancy rates, (3) the mental health Receiver plans to reassess whether further changes in pay are necessary, (4) various other efforts are underway to improve recruitment and retention, and (5) increasing compensation is a relatively costly strategy compared to other options we assess. As a result, we recommend the Legislature not provide significant across‑the‑board pay increases for mental health staff at prisons in the near term. Instead, we recommend such pay increases be considered only if the other recommendations described below and those initiated by CDCR and the Receiver prove insufficient, or if the Receiver is able to demonstrate the need for and effectiveness of further increases to support recruitment and retention. However, smaller pay increases, such as cost‑of‑living increases, or increases targeted at specific geographic regions, or providers working in specific settings, may still be appropriate in the near term.
Eliminate the Requirement for Licensed Out‑of‑State Providers to Get California Licenses. We recommend expanding the licensing exemptions so that all out‑of‑state mental health providers already licensed in their respective state no longer need to acquire a California license to work at CDCR. This exemption would eliminate the requirement for out‑of‑state mental health providers to obtain California licenses within a set amount of time of working at CDCR. Extending the exemption to all mental health providers would also allow other out‑of‑state providers who do not already have exemptions under existing state law—such as psychiatrists—to provide services if they are already licensed in another state. We also recommend directing CDCR to recruit more from out of state. To the extent feasible, similar strategies could be employed to recruit people qualified to work from other countries in cases where those countries’ licensing requirements are sufficiently similar California’s or other U.S. states. The fiscal cost of these changes would be minimal and likely absorbable, depending on how CDCR pursues greater out‑of‑state recruitment.
Increase Use of CDCR Tele‑Mental Health to Maximum Court‑Approved Levels. We recommend directing CDCR to increase the use of tele‑mental health up to the maximum levels approved by the court. This could attract qualified professionals who might not otherwise want to work in a prison setting, as well as allow the state to recruit from areas where there are more providers available. One way to implement this strategy would be to assign tele‑mental health staffing to as many CCCMS patients as possible before moving to EOP patients, given EOP patients’ greater acuity. Deploying such a strategy could also include identifying prisons that face the greatest staffing challenges and utilizing a greater share of remote workers at those facilities. The cost of increasing tele‑mental health to the maximum level allowed would be unlikely to exceed $30 million in annual ongoing costs in addition to funding for the Governor’s proposed 2026‑27 tele‑mental health expansion. These costs would come primarily from buying equipment and having sufficient on site medical assistants. CDCR, in coordination with CalHR, may need to use pay differentials for those who work inside prisons so that such providers have an incentive to remain on site. This would result in an additional fiscal cost to the state. Given that CDCR reports having more success in hiring tele‑mental health providers, we expect this expansion to reduce vacancies in the long run.
Ask Court to Allow Tele‑Mental Health Providers to Work From Out‑of‑State. We recommend the Legislature direct CDCR to request that the Coleman court remove the requirement that tele‑mental health staff work in California. This would open up a potentially large pool of new applicants who are interested in working for CDCR but would prefer not to move from their current location. Additionally, these applicants could be particularly motivated to apply given that CDCR pays more than many other out‑of‑state jurisdictions. These factors, combined with our recommendation above to waive the need to obtain California licensure, would likely increase the pool of potential staff who could work at CDCR to provide mental health services. CDCR would have to explore strategies to effectively manage such remote workers. We expect the cost of implementing this option would be largely covered by the cost of expanding tele‑mental health discussed above.
Require CDCR Report on the Feasibility of Concentrating Mental Health Population in Prisons That Are Easier to Staff. Given that it appears easier to recruit and retain mental health staff at some prisons relative to others, we recommend requiring CDCR report on the feasibility of concentrating—or clustering—the mental health population at the prisons where it is easiest to recruit and retain staff by January 10, 2027. In the report, CDCR should consider whether the lower vacancy rates at certain prisons are a result of those prisons being easier‑to‑staff and not the result of other factors that could be temporarily affecting the vacancy rate. Clustering the mental health population together could help address various challenges. For example, it could (1) make it easier to recruit staff located in areas with a wider pool of applicants, (2) reduce the need for mental health staff at locations with large vacancies, and (3) reduce the competition for mental health staff among adjacent facilities. There could be various logistical difficulties with doing this on a large scale. For example, prison infrastructure could be a limiting factor, as some prisons in easier‑to‑recruit areas may lack the appropriate space to house more mental health patients (such as sufficient housing units with medication distribution rooms to house the EOP population). Additionally, CDCR places people in prison based on a host of factors beyond their need for mental health, such as medical, rehabilitation, and security needs. Some prisons in easier‑to‑recruit areas may not be able to serve all of these other needs of some patients. Moreover, it would be important to move patients and positions between prisons so that vacancies and workload do not accumulate at prisons receiving patients in a manner that harms retention or recruitment at these prisons. Therefore, having a report that explores the feasibility and costs of concentrating the mental health population in the easiest to recruit prisons would better position the state and the Legislature to know what the challenges of such an approach are. The report should also consider how clustering could work with expanded tele‑mental health strategies, such as those discussed above. For example, the report should consider the extent to which outpatient populations could remain in hard‑to‑staff prisons but be serviced with tele‑mental health to a greater degree.
Direct CDCR to Continue to Seek Further Alignment With Bed Need Study. The Coleman court has referred CDCR’s request to deactivate a total of 249 inpatient beds to the mental health Receiver, who has so far approved the deactivations of 100 beds and is deliberating further deactivations. We recommend that CDCR request 464 further deactivations so that capacity better aligns with the bed need study. This would allow the state to reduce CDCR’s mental health funding by over $200 million if all 713 currently empty beds are deactivated without resulting in adverse effects to actual staffing or mental health services available to the incarcerated population. A reduction in inpatient beds would also reduce the number of vacancies CDCR needs to fill to comply with the Coleman court’s orders. Moreover, it would allow existing clinicians to be reassigned to fill vacancies at other prisons. This would help to reduce the strain vacancies create on the staff at those prisons—likely improving morale, recruitment and retention.
Require CDCR to Regularly Adjust Inpatient Bed Capacity. To ensure excess capacity does not accumulate in future years, we recommend directing CDCR to regularly seek adjustments to the inpatient mental health bed capacity based on the bed need study carried out biannually. To the extent the mental health Receiver denies a plan to deactivate excess bed capacity, we recommend the Legislature request from the Receiver what criteria, threshold, or buffer the state would have to achieve in order to deactivate some, if not all, of the excess capacity and direct CDCR to make changes accordingly.
Conclusion
Chronic vacancies among mental health staff in the state’s prison system are a long‑standing challenge that pose a significant risk to the wellbeing of the incarcerated population. As a result, the Coleman court has appointed a mental health Receiver to take control of the delivery of mental health services. However, the Legislature can continue to exercise oversight in this area to ensure the state is progressing toward the benchmarks specified by the courts. Accordingly, we provide a series of recommendations that would further increase the pool of potential mental health staff by expanding existing efforts in tele‑mental health and reducing barriers created by licensing requirements. We also recommend directing CDCR to further right size its inpatient capacity and develop plans to shift its mental health population to locations that would facilitate filling mental health positions. Taken together, these steps will help the state better recruit and retain mental health staff. This, in turn, could reduce the use of costly registry staff and will allow the state to better meet its constitutional requirements, lead to more effective care, and help return the mental health system to state control.