Juwan Trotter

March 18, 2026
The 2026-27 Budget
In-Home Supportive Services
- Introduction
- Background
- IHSS Costs Have Increased Over Time
- IHSS MOE Structure
- Governor’s IHSS Budget Proposals
- Other IHSS Updates
Summary
Brief Covers Drivers of In‑Home Supportive Services (IHSS) Cost Growth. Over the past couple of decades, the IHSS program has experienced significant growth in total and General Fund costs. This brief analyzes the primary drivers of cost growth in IHSS over time. Overall, IHSS has three core cost drivers: caseload, cost per hour of care, and the average hours per case. We examine how these cost drivers have changed alongside policy changes in the program and the state overall. Taken together, these cost drivers account for much of the overall growth in the program.
Maintenance‑of‑Effort (MOE) Has Resulted in State Taking On an Increasing Share of Nonfederal IHSS Costs. Historically, counties paid 35 percent of the nonfederal share of IHSS service costs and 30 percent of the nonfederal share of IHSS administrative costs. In the early 2010s, this share of cost model was replaced with an IHSS MOE. Under the MOE, county costs are adjusted annually by a fixed growth factor and a portion of locally negotiated wage increases. Part of the impetus to switch to a county MOE structure was to provide counties with fiscal relief as IHSS costs, largely outside of the counties control, continued to grow rapidly. Because nonfederal IHSS costs have grown faster than the MOE in recent years, the state has taken on an increasing share of IHSS program costs.
Governor’s Budget Includes Three IHSS Budget Solutions. In response to a projected multiyear structural deficit, the Governor’s 2026‑27 budget proposal includes three solutions in IHSS. These include (1) a proposal to eliminate the IHSS Permanent Back‑Up Provider Program (estimated to save $3.5 million in 2026‑27 and on‑going), (2) a proposal to align IHSS eligibility time lines with Medi‑Cal (estimated to save $86 million in 2026‑27 and on‑going), and (3) a proposal to remove the state’s share of cost associated with any growth in IHSS hours per case starting next year (estimated to save $233.6 million in 2027‑28, growing to $805 million in 2029‑30).
We Recommend the Legislature Ask Clarifying Questions and Weigh Trade‑Offs of Each Proposal. For each of the proposed solutions in the IHSS program, we suggest the Legislature ask the administration key, clarifying questions as it weighs the trade‑offs of each proposal. This is particularly important for the IHSS hours shift proposal, as the mechanics of how this will work remains unclear to us at this time. In particular, we note that the proposal to shift IHSS hours growth costs to counties does not assume savings until 2027‑28. This means that the Legislature has time to fully understand the proposal and its implications before taking action.
Introduction
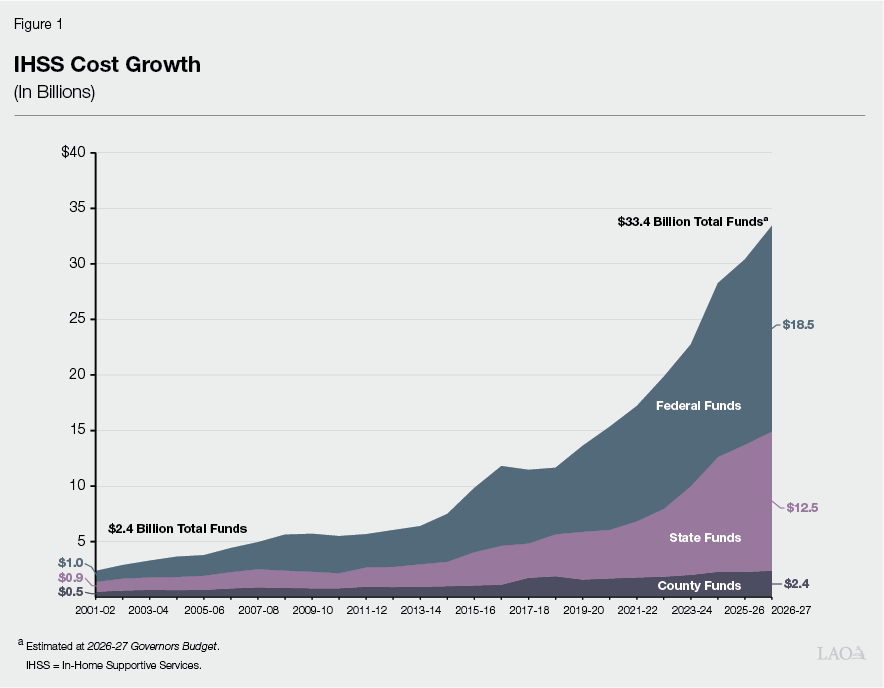
For the In‑Home Supportive Services (IHSS) program, the Governor’s 2026‑27 budget proposes approximately $12.5 billion General Fund, an increase of $1.1 billion (9.7 percent) from the Governor’s revised 2025‑26 budget estimate. This increase would bring total program funding to $33.4 billion total funds in 2026‑27 (an increase of $3 billion—10 percent—compared to revised estimates for 2025‑26). The primary drivers of this year‑to‑year General Fund cost increase include continued estimated growth in the three primary IHSS cost drivers—caseload (8 percent), cost per hour (2.3 percent), and hours per case (1.5 percent).
In light of the state’s fiscal situation (as described in the LAO publication: The 2026‑27 Budget: Overview of the Governor’s Budget), the Governor’s 2026‑27 budget also proposes three budget reductions in IHSS:
- A proposal to eliminate the IHSS Permanent Back‑up Provider Program (estimated to save $3.5 million in 2026‑27 and on‑going)
- A proposal to align IHSS eligibility time lines with Medi‑Cal (estimated to save $86 million in 2026‑27 and on‑going)
- A proposal to remove the state’s share of cost associated with any growth in IHSS hours per case starting next year (estimated to save $233.6 million in 2027‑28, growing to $805 million in 2029‑30).
This brief (1) examines IHSS cost growth and the main cost drivers over the years, (2) describes the Governor’s January 2026 proposals for IHSS, and (3) provides issues and questions for the Legislature to consider as it evaluates the IHSS budget proposals and the overall structural budget problem. We note that we are still working with the administration to better understand key aspects of the Governor’s budget proposals for IHSS. As such, this brief includes our best understanding of the proposals as of March 16, 2026. As more information becomes available, we will provide updates if necessary.
Background
Overview of the IHSS Program. The IHSS program provides personal care and domestic services to low‑income individuals to help them remain safely in their own homes and communities. In order to qualify for IHSS, a recipient must be aged, blind, or disabled, and be low income. In most cases recipients have income below the level necessary to qualify for the Supplemental Security Income/State Supplementary Payment cash assistance program (for example, about $1,234 a month for an aged and/or disabled individual living independently in 2025‑26). IHSS effectively functions as an entitlement program as all individuals who meet these requirements are eligible to receive IHSS services. IHSS recipients generally are eligible to receive up to 283 hours per month of assistance with tasks such as bathing, dressing, housework, and meal preparation. Social workers employed by county welfare departments conduct an in‑home assessment of an individual’s needs in order to determine the amount and type of service hours to be provided. In most cases, the recipient is responsible for hiring and supervising a paid IHSS provider—oftentimes a family member or relative. The average number of service hours that will be provided to an estimated 875,344 IHSS recipients is projected to be 127 hours per month in 2026‑27 (up from 125.1 in 2025‑26).
IHSS Costs Split Between Federal Government, State, and Counties. IHSS costs are shared by the federal government, state, and counties. Since IHSS primarily is delivered as a Medi‑Cal benefit, the federal share of cost is determined by the Medicaid reimbursement rate, which typically is 50 percent. The state receives an enhanced federal reimbursement rate for many IHSS recipients who receive services as a result of the Patient Protection and Affordable Care Act expansion (90 percent federal reimbursement rate) and the Community First Choice Option waiver (56 percent federal reimbursement rate). Overall, the effective federal reimbursement rate for IHSS is about 54 percent. The remaining nonfederal share of IHSS costs is covered by the state and counties. Historically, counties paid 35 percent of the nonfederal share of IHSS service costs and 30 percent of the nonfederal share of IHSS administrative costs. Beginning in 2012‑13, however, the historical county share‑of‑cost model was replaced with an IHSS county maintenance‑of‑effort (MOE), meaning county costs reflect a set amount of nonfederal IHSS costs (that may be adjusted annually by a growth factor and a portion of locally negotiated wage increases) as opposed to a certain percent of nonfederal IHSS costs. The state is responsible for covering the remaining nonfederal share of costs not covered by the IHSS county MOE.
State‑Only IHSS for Some Recipients. While the vast majority of IHSS recipients are eligible for Medi‑Cal and receive IHSS as a Medi‑Cal benefit, the state also operates the IHSS‑Residual program, which provides services to individuals not eligible for federally funded Medi‑Cal benefits, but who meet all other IHSS eligibility criteria. Beginning in 2016, the IHSS‑Residual program was also expanded over time to include individuals who are not eligible for Medi‑Cal due to their immigration status (enrollment in this population of noncitizens has since been frozen as a budget solution in 2025‑26). Because the Residual program does not receive federal financial participation, the Residual program is funded with state General Fund only.
IHSS Costs Have Increased Over Time
Given the structural budget problem, it is important to better understand the main drivers of cost increases in the state’s major programs. In this section we provide some historical information on the primary drivers of cost growth in IHSS. Overall, IHSS has three core cost drivers: caseload, cost per hour of care, and the average hours per case.
Costs of the Program Have Increased Significantly Since Fiscal Year 2001‑02… Looking back over the last couple of decades, as seen in Figure 1, the IHSS program has experienced significant growth in total and General Fund costs.
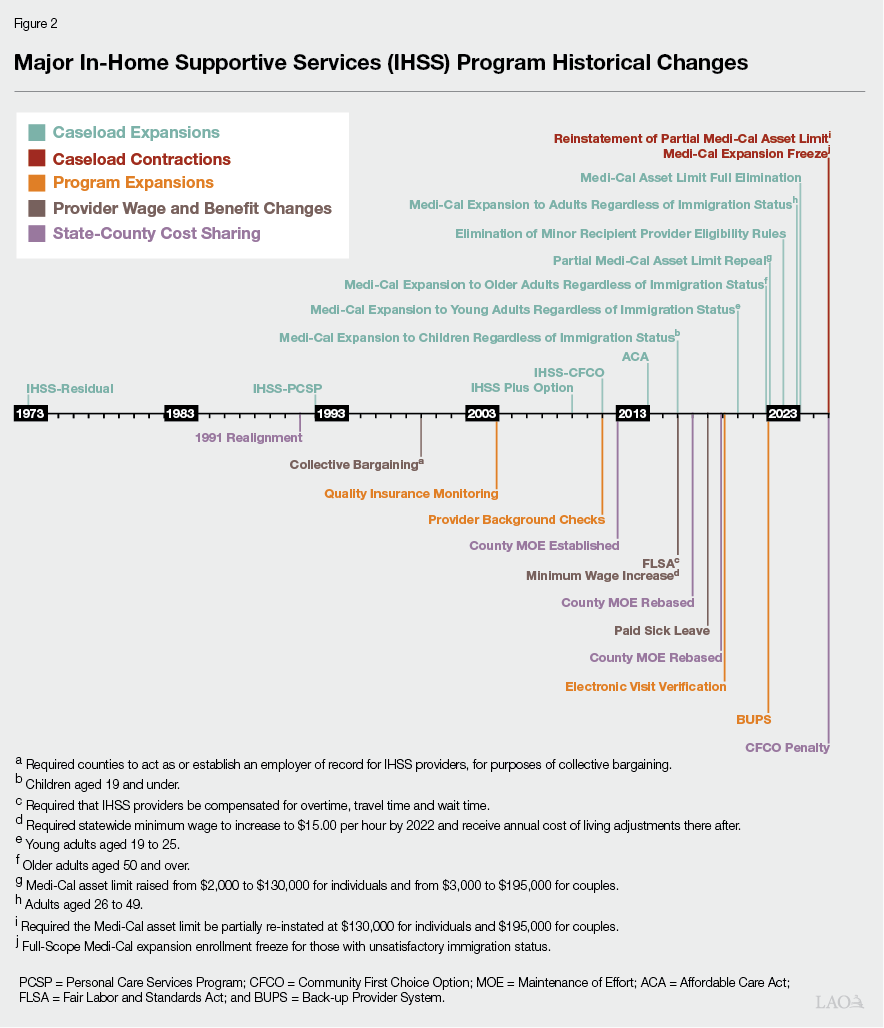
…And the Program Has Gone Through Many Historical Changes in That Time. Over this same time period, as seen in Figure 2, the IHSS program has gone through many significant policy changes (both state and federal). Notably, there has been longstanding state and federal policy that encourages a shift away from a reliance on institutional care (such as nursing homes) towards home based care (such as IHSS). For additional information on the history of the IHSS program, please refer to the Department of Social Services Website (Local Assistance Estimates for the 2026‑27 Governor’s Budget, Program History).
Primary Cost Driver: Caseload
One of the primary cost drivers in the IHSS program is caseload. When the number of people in the program increases due to underlying demographic changes or policy expansions, the cost of the program also increases. Below, we provide some background on the IHSS caseload over time.
IHSS Caseload Growth Rates Have Historically Been Variable. Although the IHSS caseload has grown at a positive rate for all but two years, since 1991‑92 (our first year of readily available data), the rate of that growth has been variable. In 1991‑92, the caseload grew at a rate of 8.1 percent. The following year (1992‑93), the caseload growth dropped to 1.4 percent. Over the next eight years, growth rates fluctuated between 3 percent and 8 percent, until reaching a peak growth rate of 10.2 percent and 10.4 percent in 2001‑02 and 2002‑03, respectively. Caseload growth then hovered between 4.5 percent and 8 percent for the next six years. However, following the passage of several service reductions, eligibility changes, and anti‑fraud initiatives, the IHSS caseload actually declined year over year by 0.2 percent in 2009‑10 and declined again by 0.02 percent in 2011‑12.
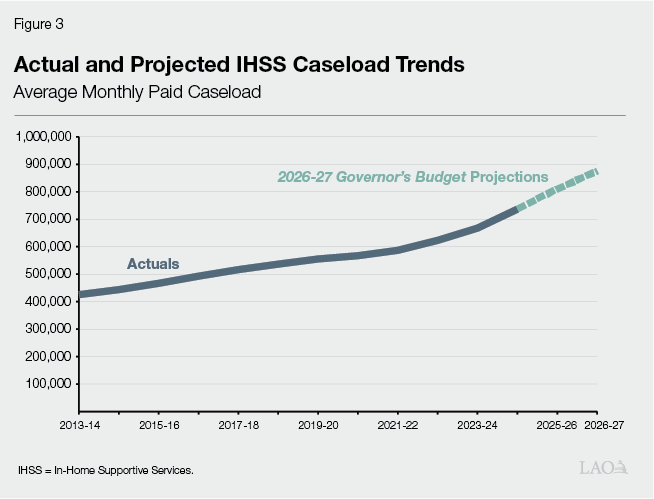
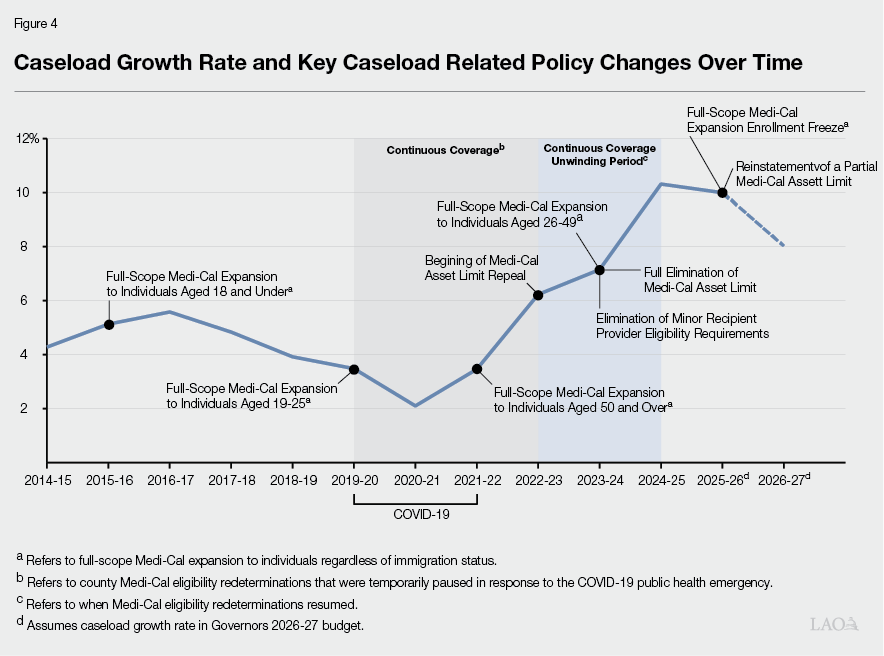
Recent Caseload Growth Has Matched Historic Highs. As seen in Figure 3, IHSS caseload has grown significantly since 2013. Despite slower caseload growth between 2016‑17 and 2020‑21 (the caseload continued to grow during this period, just at a slower than usual rate). As seen in Figure 4, the IHSS caseload growth rate has since grown at historic rates—reaching a growth rate of 10.3 percent in 2024‑25. The Governor’s 2026‑27 budget assumes the caseload will continue growing at this faster rate, estimating a growth rate of 10 percent in 2025‑26 and 8 percent in 2026‑27.
State Demographic Shifts Have Also Contributed to Increased Caseloads. While policy changes at the state and federal level have increased the number of individuals eligible to receive IHSS services, another factor contributing to the growing IHSS caseload has been the shift in state demographics. Specifically, according to the U.S. Census American Community Survey, from 2015 to 2024, the number of individuals in the state aged 65 and over has increased by 29 percent, while the overall population has increased by a little over 2 percent. Further, the number of Californians with a disability has increased by 14 percent. More specifically, those 65 and over with a disability impacting independent living has increased by 17 percent. The share of IHSS recipients over age 65, however, has remained a relatively consistent share of the overall IHSS population.
Primary Cost Driver: Cost Per Hour of Care
Another component of cost growth in IHSS is growth in the cost per hour of care. When the cost of providing care increases, for example, due to increases in the minimum wage or overtime compensation, the cost of the program also increases. Below, we take a look at how the average cost per hour of IHSS has changed over time.
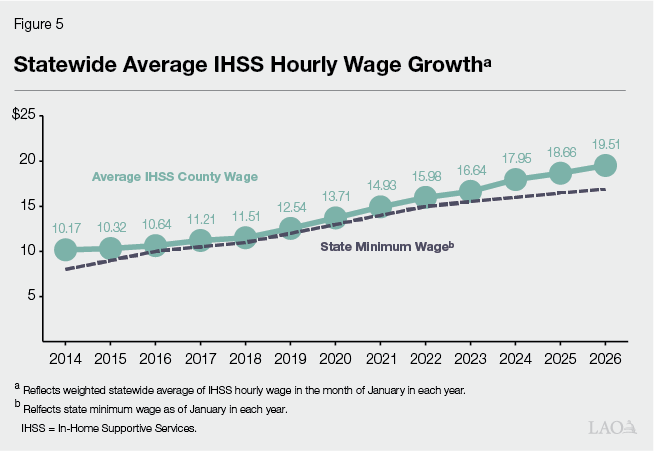
Cost Per Hour Has Increased Alongside Minimum Wage Increases. The Governor’s budget estimates that the cost per hour of IHSS services will continue to increase from $21.85 in 2025‑26 to $22.36 in 2026‑27. The IHSS cost per hour primarily includes wages but also includes other costs, such as benefits. However, as seen in Figure 5, when we consider IHSS hourly wages separately, we see that the average growth rate of hourly wages has been 5.6 percent annually since 2014. This growth in IHSS hourly wages is in part due to increases to the state minimum wage—from $8 per hour on January 1, 2014 to $16.90 per hour on January 1, 2026. Pursuant to current law, the state minimum wage will continue to increase by inflation annually (or 3.5 percent, whichever is lower). Additionally, counties may establish IHSS hourly wages above the state minimum wage through local wage ordinances or, more commonly, collectively bargained agreements. The state, federal government, and counties share the cost of IHSS wages above the minimum wage.
Primary Cost Driver: Average IHSS Hours Per Case
The next main cost driver in IHSS is the average number of hours provided per case. As the number of hours of service provided to IHSS recipients increases, so does the overall cost of the program. Below, we provide some information on how the average hours per case have changed over time.
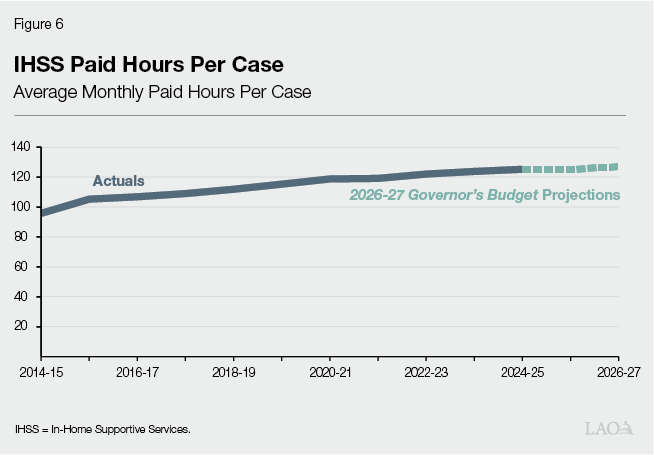
Average Hours Per Case Have Steadily Increased Over Time. As shown in Figure 6, the average monthly IHSS paid hours per case has increased by roughly 2 percent annually since 2014. The 2026‑27 budget projects the average monthly number of IHSS hours per case to increase from 125.1 hours in 2025‑26 to 127 hours in 2026‑27. We will discuss the growth in IHSS hours per case in a later section of this brief.
Taken Together, These Cost Drivers Account for Much of the Growth
Overall, IHSS Cost Growth Can Be Attributed to Three Main Factors. IHSS costs can be largely attributed to three primary factors: caseload, cost per hour, and hours per case. Between 2019‑20 and the Governors 2026‑27 budget estimate, IHSS General Fund costs are estimated to grow by about 170 percent. From approximately $4.7 billion General Fund (absent one‑time federal funds used to offset General Fund during COVID‑19) to $12.6 billion General Fund (absent the Governor’s proposed 2026‑27 IHSS reductions). Based on the available data, we believe that the primary growth factors can roughly be apportioned as follows:
- Roughly 50 percent of the growth is due to caseload growth.
- Roughly 40 percent of the growth is due to cost per hour growth (including the minimum wage increasing from $13 to $16.90, and locally negotiated wage and benefit increases above the minimum wage).
- Roughly 10 percent of the growth is due to hours per case growth.
We note that these growth components are our best estimates based on the data we have available at this time. Moreover, costs to administer the program also make up a small component of the growth listed above.
Difficult to Account for Interaction Effects. It is important to note that some of these components may be interactive, making it difficult to conclusively attribute a portion of the growth to one specific component. For example, it is possible that higher IHSS wages increase IHSS program awareness and therefore contribute to higher caseloads.
IHSS MOE Structure
The factors outlined above account for much of the growth in the overall costs of IHSS. When looking specifically at the General Fund, however, there is another structural factor that has also made it so that the above described increases are borne more by the General Fund than they were historically. In this section we outline the IHSS MOE and how it has resulted in an increasing share of IHSS program costs for the state.
Establishment of IHSS MOE. Historically, as established by the 1991‑92 State‑Local Realignment legislation, counties paid 35 percent of the nonfederal share of IHSS service costs and 30 percent of the nonfederal share of IHSS administrative costs. However, as part of the Coordinated Care Initiative (CCI), the county share of cost model—which required counties to pay a certain percent of nonfederal IHSS costs—was replaced with an IHSS MOE—which required county costs to reflect a set amount of nonfederal IHSS costs (which would be adjusted annually by a growth factor and a portion of locally negotiated wage increases). Part of the impetus to switch to a county MOE structure was to provide counties with fiscal relief as IHSS costs, largely outside of the counties’ control, continued to grow rapidly. Additionally, because CCI as envisioned shifted some program control from counties to the state, it was thought that counties should have less of a share of program costs going forward. For more information on Realignment, please see the box below. For information on the Coordinated Care Initiative, please refer to our previous report titled: The 2013‑14 Budget: Coordinated Care Initiative Update.
What Is Realignment?
Realignments Typically Shift Responsibility, and Funding, From the State to the Counties. Realignment refers to changes in program responsibility, both administrative and fiscal, between the state and counties. Typically, realignments have shifted administrative responsibility and resources from the state to counties.
1991 Realignment Adjusted County Responsibility for Health and Human Services (HHS) Program Administration and Benefits. In 1991, the state enacted a major realignment package that, among other things, increased counties’ share of cost in some programs—including In‑Home Supportive Services, while also reducing counties’ share of cost for administering other major HHS programs. Counties were also given an increased share of state revenues to cover the net increase in costs.
1991 Realignment Provided Additional Revenue to Help Pay for Increased HHS Costs. As part of 1991 Realignment, the state dedicated certain revenue sources (specifically, a new portion of the sales tax and vehicle license fee revenue) to help pay for increased HHS costs. Over time, realignment revenues were intended to cover actual program costs associated with the increase to counties’ share of cost under realignment. Under realignment, funding is allocated across different accounts that support different programs. Statute specifies which accounts (and therefore programs) should be prioritized for growth in realignment revenues and in what order.
For Realignments to Work Well, Several Principles Need to Be Met. Realignments are intended to have long‑term benefits for counties by providing (1) greater local flexibility over programs and services based on local needs and (2) incentives to encourage counties to innovate to achieve better program outcomes. Better program outcomes also benefit the state fiscally because counties’ service improvements have the potential to reduce overall costs. Moreover, with a share of cost, counties have an incentive to control program costs in areas over which they have more control (like administration). To achieve these benefits, we believe realignments need to follow certain core principles.
- Counties’ Share of Costs Reflect Their Ability to Control Costs in the Program. That is, counties’ share of cost should reflect the extent of the discretion they have over how to deliver services in the program. Programs in which the state (or federal government) set specific requirements are not good candidates for counties to have a high share of cost.
- Revenues Generally Cover Costs Over Time. While realignment revenues will not cover all county responsibilities in each year, in general, revenues should grow sufficiently to cover county costs over time.
- Flexibility to Respond to Changing Needs and Requirements. Funding allocations should be sufficiently flexible to allow counties to use funding where it is needed most.
- Funding Is Transparent and Understandable. The funding provided to counties should be easily understandable and information about the use of funding should be readily available.
Modifications to 1991 Realignment Have Been Made Over Time. Over time, as programs contained in 1991 realignment have changed, modifications have been made to the funding structure as well. For IHSS specifically, the county share of cost in the program was replaced by a set maintenance‑of‑effort. This was done in recognition of the fact that the IHSS program had changed over time and that counties no longer had the same level of control over the program. The modifications made to the counties share of program costs were made in an effort to better align the IHSS program with the principles of realignment. Specifically, they helped to better align the cost of the programs with counties available revenue and better matched counties’ costs with their level of programmatic control. For more information on 1991 realignment please see our analysis titled: Rethinking the 1991 Realignment.
MOE Structure Has Changed Over Time, Beginning With 2012 MOE. As part of the 2012 IHSS MOE, beginning in 2012‑13, all counties were required to maintain their 2011‑12 expenditure levels for IHSS, to which an annual growth factor of 3.5 percent was applied beginning in 2014‑15. Added to the MOE were any county costs associated with local IHSS wage increases. The state General Fund assumed the remaining nonfederal IHSS costs. Over the five years in which the 2012 IHSS MOE was in effect (2012‑13 to 2016‑17), growth in the county IHSS MOE was less than the growth in total IHSS costs, resulting in counties paying for a smaller share of the nonfederal IHSS costs and the state General Fund paying for a greater share of nonfederal IHSS costs relative to the original cost‑sharing ratios established under 1991 realignment. Specifically, under the 2012 IHSS MOE, the state share of IHSS nonfederal costs increased from 65 percent in 2011‑12 ($1.7 billion) to roughly 76 percent in 2016‑17 ($3.5 billion).
2017 IHSS MOE. In January 2017, CCI was ended, effectively eliminating the 2012 MOE. In response to this elimination, a new county IHSS MOE was established in July 2017—referred to as the 2017 IHSS MOE. Under the new 2017 IHSS MOE, the counties’ share of IHSS costs were reset to roughly reflect the counties’ share of estimated 2017‑18 IHSS costs based on historical county cost‑sharing ratios (35 percent of the nonfederal share of IHSS service costs and 30 percent of the nonfederal share of IHSS administrative costs). As a result of the MOE base being reset, the 2017 IHSS MOE significantly increased IHSS county costs relative to what county costs would have been under the 2012 IHSS MOE. Specifically, total IHSS county costs increased by about $630 million in 2017‑18 relative to 2016‑17. The 2017 IHSS MOE also increased annually by (1) the counties’ share of costs from locally negotiated wage increases and (2) an annual adjustment factor (of as high as 7 percent). We note that when the 2017 IHSS MOE was initially implemented, there was concern that 1991 realignment—the revenue source used to cover IHSS county MOE costs—would no longer be able to fully cover IHSS county costs in the long term. Consequently, the 2017‑18 budget agreement required the Department of Finance (DOF) to review and report on the funding structure of 1991 realignment as part of its January 2019 budget proposal. For more information on the 2017 IHSS MOE, please refer to our 2018 post titled: Recent Changes to State and County IHSS Wage and Benefit Costs.
2019 IHSS MOE. In 2019, DOF found that 1991 Realignment could no longer support the county costs of IHSS. As a result, in 2019‑20, the 2017 MOE was eliminated and replaced with the current IHSS MOE structure—referred to as the 2019 IHSS MOE. As seen in Figure 7, the 2019 IHSS MOE reduced the base county costs in 2019‑20 to roughly $1.6 billion, decreasing IHSS county costs by roughly $300 million relative to 2018‑19. The 2019 IHSS MOE was also set to increase annually by (1) the counties’ share of costs from locally negotiated wage increases and (2) an annual adjustment factor of 4 percent.
Figure 7
MOE Adjustments Over Time
|
2011 |
2017 |
2019 |
|
|
Base county cost (in billions) |
$0.9 |
$1.8 |
$1.6 |
|
Annual inflation factor |
3.5% |
As high as 7% |
4.0% |
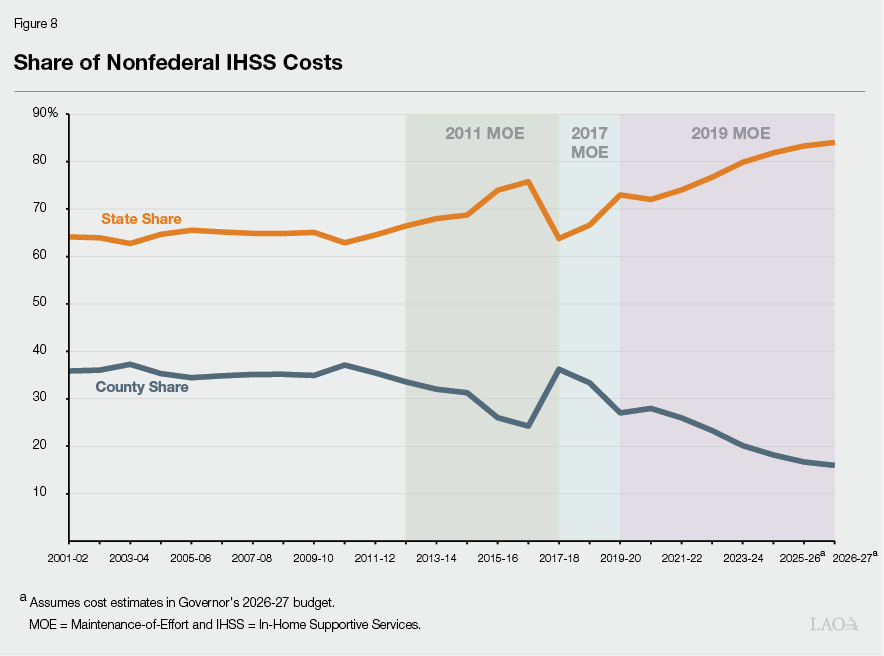
Under 2019 MOE, General Fund Costs Have Significantly Outpaced Growth in County Costs. Between 2019‑20 and 2024‑25, the annual IHSS MOE growth factor has been less than the year‑to‑year growth in total IHSS nonfederal costs. As a result, a greater share of nonfederal IHSS costs have been shifted from counties to the state. Specifically, as seen in Figure 8, under the 2019 IHSS MOE, the state share of IHSS nonfederal costs increased from 73 percent in 2019‑20 ($4.3 billion) to 82 percent in 2024‑25 ($10.3 billion).
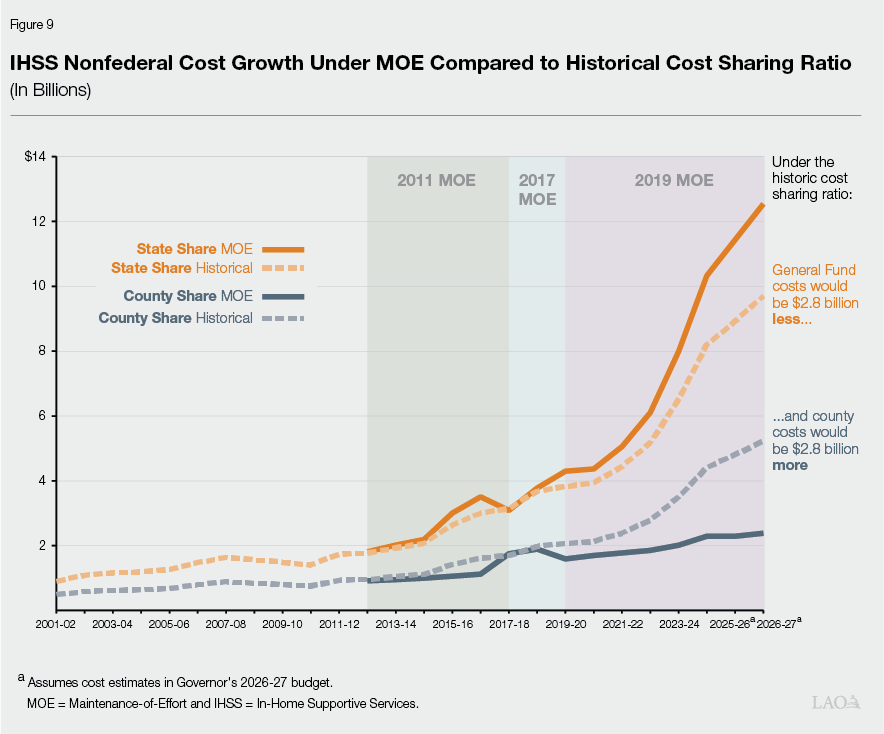
Overall, the MOE Results in the State Bearing a Larger Share of Overall Cost Increases Compared to Share of Cost Model. As seen in Figure 9, under the MOE structure, the General Fund has also taken a larger share of nonfederal IHSS costs than would have been the case under the historical share of cost model. Specifically, if the historic share of cost model had remained, the estimated 2026‑27 General Fund costs would be $2.8 billion less and estimated county costs would be $2.8 billion more.
Governor’s IHSS Budget Proposals
Recognizes Continued Growth in Primary Program Cost Drivers
Budget’s Estimates of Caseload, Cost Per Hour, and Hours Per Case Appear Reasonable. As noted in the “Introduction” section, the Governor’s budget estimates IHSS General Fund expenditures to increase by $1.1 billion (9.7 percent) between 2025‑26 and 2026‑27. This increase in costs is primarily driven by increases in each of the programs three primary cost drivers—caseload (8 percent), cost per hour (2.3 percent), and hours per case (1.5 percent). Overall, we find that the Governor’s budget estimates for these primary cost drivers appear reasonable. We will continue to monitor actual caseload, cost per case, and hours per case data and provide updates, as needed, at the May Revision. Below, we present the Governor’s three reduction proposals for the IHSS program and provide issues and questions for the Legislature to consider as it evaluates these proposals.
Elimination of Permanent Back‑Up Provider System
Permanent Back‑Up Provider System (BUPS) Established in 2022‑23 Budget. The 2021‑22 budget included $5 million General Fund to create a permanent IHSS back‑up provider system on January 1, 2022, contingent on a policy framework being adopted in statute. However, a policy framework for the BUPS program was not adopted within the 2021‑22 budget period, resulting in the initial $5 million allocation going unspent. The 2022‑23 budget codified a policy framework for BUPS. Under BUPS, a recipient whose regular provider is not available, but who has an urgent need or whose health and safety will be at risk without a back‑up provider, can receive up to 80 hours (if the recipient is non‑severely impaired) or 160 hours (if the recipient is severely impaired) of back‑up provider services per fiscal year. Additionally, back‑up providers are paid $2 above the local IHSS hourly wage rate.
Utilization of Back‑Up Provider System Has Fallen Below Expectations Since Inception. As seen in Figure 10, the 2023‑24 Budget Act appropriated a total of approximately $18.4 million General Fund ($15.7 million for services, $2.7 million for administration) for BUPS. From October 2022 through June 2024 (the most recent month of available expenditures), less than $900,000 total funds had been spent on Back‑Up Provider services. Because utilization in 2023‑24 was lower than expected, the 2024‑25 Budget Act appropriation was reduced to approximately $8.6 million General Fund ($5.6 million for services, $3 million for administration). However, the Governor’s 2026‑27 budget includes updated estimates that BUPS will cost $4.5 million General Fund in fiscal year 2025‑26. Most of the funding in 2025‑26 is estimated to go towards administering the program ($4.2 million) rather than the services themselves ($298,000). It is our understanding from the administration that the decreasing service costs reflect updated utilization estimates; however, we are continuing to explore the reasons estimated administrative costs for the program remain elevated relative to estimated service costs.
Figure 10
Back‑up Provider System Allocations Over Time
(In Millions)
|
Services |
Administration |
Total |
|
|
2023‑24a |
$15.7 |
$2.7 |
$18.4 |
|
2024‑25b |
5.6 |
3.0 |
8.6 |
|
2025‑26c |
0.3 |
4.2 |
4.5 |
|
a2023‑24 Budget Act appropriation. b2024‑25 Budget Act appropriation. cEstimate at 2026‑27 Governor’s Budget. |
|||
Governor’s Budget Proposes to Eliminate State Back‑Up Provider System. The Governor’s budget proposes to eliminate the BUPS program, resulting in an estimated $3.5 million General Fund savings in fiscal year 2026‑27 and ongoing.
Some Counties Had Local Back‑Up Provider Programs Prior to Establishment of State System. It is our understanding from speaking with county Public Authorities, that prior to the establishment of the statewide BUPS program, multiple counties had established their own local back‑up provider programs—some of which continued to run alongside the statewide system. For example, the Los Angeles County Public Authority has and continues to run the Back‑Up Attendant Program (BUAP) alongside the statewide BUPS program. While similar to BUPS, BUAP requires a recipient to have a minimum of 25 hours per week (BUPS has no minimum hour requirement), requires providers to have additional experience or certification compared to BUPS, and pays $3 above the local wage (BUPS pays $2 above the local wage).
Key Questions for Legislative Consideration. Given the current budget challenges, and the notable low utilization of the program, the Legislature may wish to consider the trade‑offs associated with this proposal. In doing so, the Legislature could ask the administration the following questions:
- What have been the main challenges that have led to the lower‑than‑initially‑expected utilization of the program?
- Is lower‑than‑expected utilization due to challenges in finding available providers? Does the administration have information on how often a back‑up provider is requested but not provided?
- Are there ways to reduce the administrative costs? Could a more centralized model be considered?
- Are there opportunities for the state to better support local county back‑up programs?
- Last year, the administration indicated it was going to work to educate and inform more recipients of the program. Did that effort ever occur?
Conform IHSS‑Residual Program With Medi‑Cal Coverage
IHSS‑Residual Serves Individuals Not Eligible for Medi‑Cal… As noted in the “Background” section of this brief, the vast majority of IHSS recipients are eligible for Medi‑Cal and receive IHSS as a Medi‑Cal benefit—allowing the state to draw down federal funds to offset state IHSS costs. However, the state also operates the IHSS‑Residual program, which provides services to individuals not eligible for federally funded Medi‑Cal benefits, but who meet all other IHSS eligibility criteria. Costs for the IHSS‑Residual program are fully covered by the state. Currently, the vast majority of those who enter the IHSS‑Residual program are either (1) individuals who are not eligible for Medi‑Cal due to their immigration status or (2) recipients who were terminated from Medi‑Cal due to noncompliance (for example, failing to submit Medi‑Cal re‑determination paperwork).
…However, IHSS Recipients Who Do Not Comply With Medi‑Cal Eligibility Rules May Be Treated Differently. The consequences for IHSS recipients terminated from Medi‑Cal due to Medi‑Cal noncompliance currently varies. In some counties, these recipients may also be terminated from IHSS because IHSS is a benefit of Medi‑Cal. In other counties, these individuals may fall into the IHSS‑Residual program as a sort of “safety net” until they get their Medi‑Cal reestablished. Whether a recipient is manually terminated from IHSS or is enrolled in the IHSS‑Residual program is entirely dependent on the practices in the county they reside in.
- Some Cases Get Transferred to the IHSS‑Residual Program. If a recipient terminated from Medi‑Cal is not manually terminated from IHSS the recipient is automatically enrolled into the IHSS‑Residual program until the county worker updates the case. While this means that a recipient’s provider continues to receive service payments in real time, the state General Fund is responsible for covering all costs and cannot draw down federal funds until the recipient is reenrolled into Medi‑Cal. Currently, as we understand it, there is no statutory limit to how long an IHSS recipient may remain in the IHSS‑Residual program. Additionally, it is our understanding that the state cannot retroactively draw down federal funds for payments made through the IHSS‑Residual program during the recipient’s gap in Medi‑Cal eligibility.
- Some Cases Are Manually Terminated From IHSS. If an IHSS recipient terminated from Medi‑Cal is manually terminated from IHSS, the recipient needs to reinstate their Medi‑Cal eligibility in order to receive paid services through the IHSS program again. As a result, if a recipient’s provider continues to provide care, they will not receive payments for services until the recipient reinstates their Medi‑Cal eligibility. Once the recipient reinstates their Medi‑Cal eligibility, they are eligible to return to IHSS. Additionally, if Medi‑Cal eligibility is re‑instated within 90 days of termination, the state can retroactively draw down federal funds and pay IHSS providers for services provided during the gap in IHSS and Medi‑Cal eligibility.
Administration’s Interpretation of IHSS‑Residual Eligibility Rules. Under current statute, individuals eligible for federally funded Medi‑Cal benefits are ineligible for the IHSS‑Residual program. Only individuals not eligible for federally funded Medi‑Cal benefits are eligible to receive services through the IHSS‑Residual program. The administration’s interpretation of statute is that individuals who were once eligible for federally funded Medi‑Cal benefits, but were terminated from Medi‑Cal due to noncompliance, are ineligible for the IHSS‑Residual program.
Governor Proposes to Automate Termination of IHSS Concurrent With Medi‑Cal. As part of the proposed 2026‑27 budget, the Governor proposes to automate the IHSS termination process for individuals who are terminated from Medi‑Cal. This would ensure that recipients who are terminated from Medi‑Cal due to Medi‑Cal noncompliance will be automatically terminated from IHSS and not be enrolled in the IHSS‑Residual program. As a result, some recipients who may have been enrolled into the IHSS‑Residual program—allowing them to continue to receive IHSS services through this state funded program—would no longer receive IHSS services once terminated from Medi‑Cal. Additionally, unlike current practice, this proposal would ensure that all recipients who are terminated form Medi‑Cal due to noncompliance would be treated the same regardless of the county in which they reside. This proposal would not impact recipients who utilize the IHSS‑Residual program due to their immigration status.
Implementing This Proposal at the Same Time as Upcoming Federal Changes May Present Additional Challenges. Currently, Medi‑Cal generally renews eligibility for beneficiaries every 12 months. However, beginning in January 2027, as a part of the new federal requirements of H.R. 1, the state will be required to renew eligibility every six months for recipients within the Medicaid expansion population under the Patient Protection and Affordable Care Act (ACA)—generally childless adults. The increased frequency of redeterminations will increase the risk these IHSS recipients lose Medi‑Cal coverage. Under the Governor’s proposal, these individuals would also be automatically terminated from IHSS. The Governor’s budget estimates the IHSS ACA population to consist of roughly 42,000 average monthly cases in 2025‑26.
Governor’s Budget Assumes All Terminated Cases Would Reinstate Medi‑Cal and IHSS Eligibility. Under the administration’s proposal, it is our understanding that recipients would be automatically reenrolled into IHSS if they reinstate their Medi‑Cal eligibility within 90 days. (Recipients would be manually reinstated into IHSS if they reinstate their Medi‑Cal eligibility after 90 days.) The Governor’s budget assumes all recipients would be reinstated into Medi‑Cal and IHSS within 90 days of termination and assumes all recipients would continue to receive services during the gap in eligibility and providers would be retroactively reimbursed once the recipient is reenrolled into Medi‑Cal and IHSS. As such, rather than the state paying for all service costs through the IHSS‑Residual program, the administration estimates the state would be able to draw down federal funds to cover a portion of these service costs. As a result, the Governor’s budget includes $86 million net General Fund savings in 2026‑27 and ongoing.
Alternatives to Governor’s Proposal. This proposal has been before the Legislature (and rejected) a number of times over the years. As such, the Legislature may wish to consider the alternatives to the Governor’s proposal as well as options that could mitigate the impacts of the proposal, were it adopted. It should be noted, however, that most of these alternatives would not save as much as the Governor’s proposed change (and may, in some cases, result in up‑front costs).
- Better Communication to Recipients. Currently, it is our understanding that when IHSS recipients receive Medi‑Cal re‑determination materials or a notice of Medi‑Cal termination, it may not be fully understood that losing Medi‑Cal eligibility would also mean potentially losing IHSS services. As such, providing a clear written warning that any loss of Medi‑Cal eligibility could result in a loss of IHSS services may decrease the number of IHSS recipients losing Medi‑Cal eligibility due to noncompliance. (This alternative could be adopted alone or alongside the Governor’s proposal to mitigate disenrollments.)
- Provide Administrative Funding to Prevent Medi‑Cal Disenrollments. By providing county administrative staff with additional resources, counties may be better positioned to assist and provide outreach to IHSS recipients at risk of losing Medi‑Cal eligibility. This could prevent IHSS recipients from losing Medi‑Cal eligibility due to noncompliance. Or, if an IHSS recipient has been terminated from Medi‑Cal, increased resources could allow county administrators to better assist recipients in re‑enrolling into Medi‑Cal on a timely basis—increasing the chances of retroactive payment and federal funding participation. (This proposal could be adopted alone or alongside the Governor’s proposal to mitigate disenrollments.) As we discuss in our recent report, The 2026‑27 Budget: County Administration and H.R. 1 Administration, the Legislature may also want to decide to weigh the trade‑offs of providing additional funds to counties to mitigate disenrollments related to H.R. 1 implementation. (The key trade‑off being what alternative solutions to adopt in order to free up resources to support additional funding for counties.)
- Exclude Certain Populations From Automatic Termination. Certain IHSS recipients—for example, those with a high level of authorized hours—may have greater difficulty completing the administrative tasks required to remain in compliance with Medi‑Cal. Excluding this population from the Governor’s proposal may avoid adding undue hardship on those who require IHSS services the most and who would also likely have the greatest difficulty re‑enrolling into Medi‑Cal should they be terminated.
- Allow for a Standardized Grace Period. Currently, when an individual is terminated from Medi‑Cal for noncompliance, they may be manually terminated from IHSS immediately, enrolled in IHSS‑Residual for a period of time before being terminated from IHSS, or allowed to remain in the IHSS‑Residual program indefinitely. An alternative to automatically terminating all IHSS recipients when they lose Medi‑Cal eligibility (as proposed by the Governor) could be to allow all recipients who are terminated from Medi‑Cal for noncompliance to enroll in IHSS‑residual for a certain period of time (for example six months) before being terminated from IHSS. This would allow recipients extra time to re‑enroll into Medi‑Cal before being terminated from IHSS. We note, however, that this alternative would result in less savings than the Governor’s proposal, and could possibly result in no savings or additional costs compared to the status quo. This is because some counties currently terminate IHSS recipients immediately and requiring those counties to allow recipients to remain in the IHSS‑Residual program for longer than they otherwise would have would result in those cases costing more than is the case today.
Current Statute Is Not Clear on Whether Recipients Terminated From Medi‑Cal Are Ineligible for IHSS‑Residual Program. As previously mentioned, the administration interprets current statute as rendering recipients terminated from Medi‑Cal ineligible for the IHSS‑Residual program. Despite the administration’s interpretation, we understand that counties may have a different understanding of the statute—leading to varying usage of the IHSS‑Residual program throughout the state. Specifically, current statute mentions that individuals ineligible for federally funded Medi‑Cal benefits are eligible for the IHSS‑Residual program. If an individual is terminated from Medi‑Cal due to noncompliance, it can be reasonably understood to mean the individual is ineligible for federally funded Medi‑Cal benefits. Consequently, it is unclear to us whether that individual could be eligible for the IHSS‑Residual program.
Legislature Should Consider Clarifying Purpose of IHSS‑Residual Program. If the Legislature does not adopt the Governor’s proposal, it is likely that the current variance in the usage of the IHSS‑Residual program would continue. That is, some counties would continue providing services through the IHSS‑Residual program even after Medi‑Cal coverage is terminated, while some counties would continue to terminate recipients from IHSS to align with their Medi‑Cal status (similar to the Governor’s proposal). This raises equity issues, as recipients would be treated differently only based on the county in which they live. The Legislature may want to consider what the role of the IHSS‑Residual program should be. Regardless of whether the Legislature adopts the proposed change, we recommend amending statute to clarify whether individuals ineligible for federally funded Medi‑Cal benefits due to Medi‑Cal noncompliance are or are not eligible for the IHSS‑Residual program. Such clarification will increase the likelihood that the policy is implemented consistently throughout the state. Additionally, the Legislature may want to consider how long recipients would be permitted to remain in the IHSS‑Residual program and whether recipients would be manually or automatically terminated from the IHSS‑Residual program if the recipient does not reinstate their Medi‑Cal eligibility within the specified time frame.
Additional Issues for Consideration if Legislature Adopts Governor’s Proposal. While the administration assumes all recipients would continue to receive services during the gap in Medi‑Cal and IHSS eligibility (and providers would be retroactively reimbursed), some recipients may experience a disruption in care and not return to Medi‑Cal and IHSS. Thus, should the Legislature adopt some version of the administration’s proposal, it may want to consider asking the administration to monitor and report back on (1) how long it takes recipients to reinstate their Medi‑Cal and IHSS eligibility, (2) the extent to which recipients experience a disruption in care, and (3) the number of recipients who ultimately do not return to Medi‑Cal or IHSS. With that data, the Legislature could consider tailoring the policy in the future in order to maintain services for eligible IHSS recipients.
Remove State’s Share of Cost in IHSS Hours Per Case Growth
As noted at the start of this brief, the average hours per case for IHSS has been steadily increasing for many years. This has been a factor in the overall growth in program costs over time. Below, we present how counties assess IHSS hours, what we know of the Governor’s proposal to date, and potential alternatives and outstanding questions for the administration.
How Are IHSS Hours Assessed Today?
What Is an IHSS Functional Index Ranking? When an IHSS social worker conducts an assessment, they rank the recipient’s impairment to perform activities of daily living on a six‑point scale known as the functional index (FI) ranking. An FI ranking of 1 is the lowest impairment level and notes that a recipient is independent and able to perform a task without another person’s assistance. An FI ranking of 5 notes that a recipient cannot perform a task with or without another person’s assistance and an FI ranking of 6 signifies a recipient requires paramedical services (meaning that, in order to provide the service, a provider must be trained and overseen by a licensed health care professional). The weighted average of the FI rankings for each assessed task are then used to create an overall FI score. For minor recipients, there is a separate age appropriate guidelines tool where FI ranks are adjusted to reflect the age at which a minor may be expected to complete a task. For example, when assessing a minor below the age of 14 for laundry services, rather than assessing the recipient’s level of need based on the regular six point FI scale, social workers assess an FI ranking of 1 unless there is extraordinary need above what would be required for a minor who does not require IHSS services. This is because the age appropriate guidelines tool regards laundry services provided for a minor aged 14 and under to be within the expected responsibilities of a parent or guardian.
What Are the Hourly Task Guidelines (HTG)? County social workers then use the Hourly Task Guidelines to determine the amount of hours to authorize for each IHSS task. The time required is determined based on the recipient’s FI ranking, as well as other considerations including the recipient’s living environment. For FI rankings 2 through 5, there is a range of hours that can be allocated depending on the nature of the assistance needed. For example, the hours assigned for the task of meal preparation not only depend on the severity of the recipient’s assessed impairment but also the type of food the recipient usually eats; whether those meals are pre‑packaged, cooked, or can be re‑heated; and the frequency with which the recipient eats. Because of this, a recipient with an FI ranking of 3 for meal preparation, for example, may be authorized hours ranging from 3.3 to 7 hours per week. For an FI ranking of 6, a licensed health care professional will indicate the amount of time necessary to perform the specific task.
The HTG Allows for Flexibilities in Authorized Hours. Further, there are service categories where different FI ranks may have overlapping ranges of hours under the HTG. For example, as seen in Figure 11, a recipient with an FI rank of 2 may be assigned a greater number of hours than a recipient with an FI rank of 4 for certain tasks. In this case, a recipient with an FI rank of 2 may be physically able to prepare their own meals but may move slowly and require constant prompting and encouragement, while a recipient with an FI rank of 4 may rely totally on their caregiver to cook but may be able to use a microwave and consume premade meals. In this case, the person with the FI ranking of 4 may receive very similar hours for meal preparation as the person with an FI rank of 2. Exceptions may also be made to allow a recipient to live safely and independently in their own home. An example of an exception that may require more time than what is prescribed by the HTG is if a recipient has a dietary restriction that requires longer preparation times or more frequent meals. Alternatively, if a recipient eats relatively simple meals (for example toast and coffee for breakfast) they could receive below the minimum amount of time prescribed by the HTG.
Figure 11
Hourly Task Guideline for Meal Preparation
|
Functional Index Ranking |
Range of Hours |
|
|
Low |
High |
|
|
Rank 2 |
3.01 |
7.00 |
|
Rank 3 |
3.30 |
7.00 |
|
Rank 4 |
5.15 |
7.00 |
|
Rank 5 |
7.00 |
7.00 |
Protective Supervision Increases Hours, but Not FI Scores. Some IHSS recipients are determined to require “protective supervision” to remain safely in their own homes. Protective supervision allows certain recipients to receive the maximum amount of hours allowed to them (195 hours if non‑severely impaired, 283 hours if severely impaired). To receive protective supervision, an IHSS recipient must be deemed non‑self‑directing, meaning that because of their mental impairment or mental illness, the recipient does not understand what is dangerous, and may be more likely to perform dangerous actions that could cause them to get hurt. They must also be assessed to need 24‑hour‑a‑day supervision to remain in their home safely and these needs must be certified by a medical professional. It should be noted that recipients determined to need protective supervision do not receive an FI ranking for protective supervision. As such, while a recipient’s overall FI score does not change whether or not they are provided protective supervision services, their hours would be quite different.
Department of Social Services (DSS) Conducts Quality Assurance Monitoring. DSS works with counties to conduct quality assurance monitoring. These tasks include, but are not limited to, conducting home visits, reviewing Case Management Information and Payrolling Systems data, and case reviews—including reviewing FI rankings and HTG exceptions. The administration has also noted that they have recently conducted a statewide refresh training for all county staff on the use of these assessment tools. We are working with the administration to better understand this recent quality assurance effort and the outcomes of the statewide refresh training.
There Is Variance in the Average Hours Per Case by County. Although there are standardized tools and quality assurance measures in place, there is variance in the average hours authorized per case. Average hours per case vary widely throughout the state, estimated to range from a high of 170.7 hours per case in Mono County to a low of 86.6 hours per case in Trinity County in 2025‑26. There are many reasons why this could potentially be the case. For example, it remains unclear if counties with higher average hours per case also tend to have recipients with greater needs and higher average FI scores. Additionally, as noted previously, demographics within the state continue to change. Recipient needs may be growing as the population ages, and these changes may not be happening equally across the state. The reason for this variance is something we are currently working with the administration to better understand.
Governor’s Proposal
Governor Proposes to Shift Costs Associated With Growth in IHSS Hours Per Case to Counties Beginning in 2027‑28. As noted earlier in this brief, current growth in the hours per case is something that is paid for by the state and federal governments. Counties currently do not experience added costs (above the annual 4 percent growth in county costs built into the county MOE) when hours per case grow. Beginning July 1, 2027, the Governor proposes to shift nonfederal costs associated with any increase in average hours per case to the counties. The administration estimates that this proposal would save approximately $233 million General Fund in 2027‑28 and grow to over $800 million General Fund savings in 2029‑30.
Mechanics of Governor’s Proposal Remain Unclear. Although the administration is clear that the concept of this proposal, at a high level, is to shift the cost of increases in the average hours per case from the state to the counties, the mechanics of how this would actually work remain unclear to us at this time. In order to fully analyze the proposal, it will be necessary to receive further details from the administration. Below, we describe two main ways such a shift has been described to us to date:
- Only Counties Above the Statewide Average Pay for Hour Growth. As described in the trailer bill language released in February 2026, the administration’s proposal would require the administration to calculate a statewide annual baseline level of authorized hours per case. The language would then require any county with average authorized hours above the baseline to pay 100 percent of the nonfederal cost of any growth in their average authorized hours. This would mean that any growth in hours per case that occurs in the counties below the statewide average baseline would still receive General Fund support.
- All Counties Share in the Cost of Growth in Average Hours Per Case. After speaking with the administration, however, we understood their vision of the proposal to differ from that described in the trailer bill. At a high level, based on that conversation, it is our understanding that the Governor’s proposal would similarly require the administration, each year, to calculate a statewide average authorized IHSS hours per case baseline. However, the costs associated with any growth in statewide average authorized hours per case above this baseline would then be shifted to all counties to pay in proportion to their share of the overall IHSS caseload. This means that all counties would be required to pay a portion of this growth in statewide average authorized hours per case, regardless of whether the county has average hours per case growth above the baseline average or not.
The administration recently informed us that it continues to work through the mechanics of how this proposal would function. We will continue to work with the administration to clarify this proposal and will provide updated information as necessary.
No Changes to HTGs or How Assessments Are Conducted… Although the actual mechanics of how this proposal would be implemented are unclear at this time, the administration has been clear that this proposal would have no impact on the current hourly task guidelines or FI ranking process. Moreover, it would not prohibit increases in hours assessed as necessary by social workers.
…Or the Existing MOE. The administration has also been clear that this proposal would have no impact on the current MOE structure. All costs that are shifted from the General Fund to the counties in relation to this proposal would lie outside of the established MOE agreement that is currently in place.
Administration’s Rationale for Shifting Costs to Counties. The administration has provided several rationales for this proposal. However, primarily the administration has made one key point—because counties control and perform IHSS assessments, giving them a direct fiscal responsibility for the growth in hours per case will incentivize counties to ensure accurate assessments. As context for this proposal, the administration has noted that, since the establishment of the 2019 MOE, the state has been taking on an increasing share of nonfederal IHSS costs. This proposal would shift the cost of some of this growth back onto the counties. Below, we lay out some of our concerns for consideration.
Administration Has Not Assessed the Root Cause of Variance in Hour Authorizations Across the State. The administration has noted that over the past several years, the statewide average authorized hours per case has increased while the statewide average FI score has remained relatively flat. While we are working with the administration to better understand the data being utilized to substantiate this claim, it remains unclear if the statewide average authorized hours per case is the best metric for determining whether IHSS hours are being accurately assessed by the counties. Additionally, the growth rate for hours per case has remained relatively steady over time. As such, whether any particular state policy changes have impacted the growth rate is unclear.
Mechanics of Governor’s Proposal Are Important to Understand County Ability to Control Costs. Depending on how this proposal is operationalized, counties will have differing levels of control over their costs. For example, if the costs associated with any growth in authorized hours per case is applied to all counties in proportion to their share of the overall IHSS caseload, then counties will have little to no control over their own costs. This is because the amount a county will pay under this version of the proposal depends on a county’s share of the IHSS caseload and not whether the county increased authorized hours. Meaning, a change in an individual county’s average hours per case will have little impact on the amount their costs will grow. For example, under this interpretation of the proposal, a disproportionate share of the cost (35.5 percent in 2025‑26) would fall onto Los Angeles County, despite Los Angeles County having one of the lowest average authorized hours per case in the state (118.8 hours per case) and an average hours per case well below the statewide average (125 hours per case). Further, a majority of the state’s IHSS caseload is concentrated amongst a small number counties, but these counties do not necessarily have the highest average authorized hours per case.
Alternatively, if the costs associated with the growth in authorized hours per case is applied only to those counties above the statewide average hours per case, the proposal may better align with a county’s ability to control their own costs. This is because, particularly for those counties close to the statewide average hours per case baseline, counties able to shift their average hours per case below the statewide average will not have increased costs. That said, we are uncertain of the level of control counties have to change their average authorized hours per case since they rely on standardized tools and assessment processes. Depending on how statewide average hours per case change in relation to this proposal, General Fund savings may differ than what the administration currently estimates.
Shifting These Costs to Counties Would Not Fundamentally Change the Share of Costs Borne by the Counties Compared to the State, but Would Erode Purpose of the MOE. As described in the “IHSS MOE Structure” section of this brief, over time, the state has been taking on a larger share of nonfederal IHSS costs compared to the counties. As was noted, however, the establishment of an MOE structure in IHSS was in recognition of the counties previously having a share of cost in the program that was determined to be too high compared to their level of programmatic control. The MOE was meant to better align counties’ share of cost in the program with their level of programmatic control—a key feature of a successful realignment. Although the cost shift associated with this proposal is significant for counties, it would not fundamentally change the overall share of cost borne by the counties compared to the state. Specifically, the administration’s estimated $233 million in costs being shifted from General Fund to the counites in 2027‑28 as a result of this proposal equates to only 2 percent of the nonfederal share of IHSS costs. Finally, making incremental adjustments to counties’ costs in the program, without impacting the MOE, does raise questions about the purpose and value of the MOE.
Legislature Has Time to Evaluate Proposal Before Proposed 2027‑28 Implementation. The Governor’s proposal would not begin until fiscal year 2027‑28—meaning the 2026‑27 budget does not assume any savings from the proposal. This gives the Legislature additional time to ask questions and gain clarity on this proposal before making a decision. With this additional time, and given the fundamental questions that remain, we suggest the Legislature ask the administration the following questions:
- Mechanics of the Proposal. How would this proposal be implemented? Would it impact all counties or only counties above the statewide average hours?
- Evidence Around Average Hour Per Case Increase. What evidence does the administration have that the average hours per case is growing faster than would be expected or needed? Are there certain populations, for example, certain ages or certain tasks, such as protective supervision, that seem to have the most growth?
- Has the Administration Considered Other Options to Address Hour Increases? Since the FI rankings and the HTGs are tools provided to counties by the state, the counties have limited control over how to apply them. Has the administration considered whether the tools themselves (or the state’s oversight of the tools) should be reevaluated?
- Does It Make Sense to Incrementally Increase County Costs Outside of the MOE? Or would it make more sense to take a more holistic view of how county and state shares of costs in the program have changed over time? It has been nearly ten years since the most recent MOE was established. Is it working as intended? Should adjustments be considered?
- Are Counties Able to Absorb Increased Costs With Current Level of 1991 Realignment Revenues? As noted earlier, realignment works best when counties’ revenue generally cover costs over time. The MOE that is currently in place was an attempt to better meet this principle. Has the administration worked with the counties to determine the level of increased costs counties would be able to bear with 1991 realignment revenue? How would an increase in county IHSS costs impact counties’ ability to fund other social services programs with realignment revenue?
Other IHSS Updates
Community First Choice Option (CFCO) Penalty Update. CFCO is a federal program within IHSS that is aimed at serving those with the highest needs for assistance in their homes. The IHSS cases eligible for the CFCO program receive the regular base Federal Medical Assistance Percentage (FMAP) of 50 percent, plus an additional enhanced FMAP of 6 percent (for a total FMAP of 56 percent). However, if counties do not conduct timely, federally required reassessments of CFCO recipients, those particular cases are no longer eligible to receive the additional 6 percent FMAP. The cost of this lost 6 percent FMAP must then be reimbursed to the federal government. Since 2017, the cost of this lost 6 percent FMAP (also referred to as the CFCO late penalty) has been paid for with the General Fund and has grown over time—totaling $63.2 million in 2023‑24.
The 2025‑26 Budget Act shifted half of the cost of the CFCO late penalty to counties in 2025‑26 (estimated in Governor’s budget to save $40.5 million General Fund) and the full cost of the CFCO late penalty beginning in 2026‑27 and ongoing. The Governor’s budget estimates the savings to be $92 million General Fund in 2026‑27. However, if counties comply with the CFCO reassessment requirements, they will not incur a penalty and will therefore not have additional costs.
Timely CFCO Reassessments May Come at the Expense of Other County Workload Priorities. Currently, it is our understanding from speaking with counties that the number of CFCO cases in noncompliance has decreased since the enactment of this policy, and as such, the cost to the counties, as a result of this policy, may be lower than the Governor’s budget estimates. However, it is also our understanding from speaking with counties, that potentially as a result of counites shifting workload to prioritize the reassessment of CFCO cases, the number of applications that take over 90 days to be processed has grown from 1,600 to 4,600 in the first six months of the CFCO penalty policy being in effect.