Karina Hendren

March 13, 2026
The 2026-27 Budget
Department of Developmental Services
Summary
The Department of Developmental Services (DDS) coordinates a wide variety of services for about 490,000 Californians with intellectual and developmental disabilities or similar conditions. In this brief, we provide some basic background on DDS, then describe and assess the Governor’s 2026‑27 budget proposal for the department. The Governor’s budget proposes one‑time funding to continue planning for an information technology (IT) project that aims to modernize the program’s case management and accounting systems. The budget also proposes ongoing funding to support compliance with a recently enacted federal rule. These proposals total just under $8 million General Fund.
We also address ongoing oversight and implementation issues in the context of a changing fiscal and policy landscape. Specifically, we provide background and issues for legislative consideration on the following areas: (1) implementation of H.R. 1, federal legislation enacted in July 2025 that affects Medicaid funding; (2) progress on service provider rate reform and the quality incentive program; and (3) DDS spending trends over the last several years and underlying cost drivers.
Background
Lanterman Act Lays Foundation for “Statutory Entitlement.” California’s Lanterman Developmental Disabilities Services Act (Lanterman Act) originally was passed in 1969 and substantially revised in 1977. It amounts to a statutory entitlement to services and supports for individuals ages three and older who have a qualifying disability. Qualifying disabilities include autism, epilepsy, cerebral palsy, intellectual disabilities, and other conditions closely related to intellectual disabilities that require similar treatment, such as a traumatic brain injury. To qualify, an individual must have a disability that is substantial, expected to continue indefinitely, and which began before the age of 18. There are no income‑related eligibility criteria. As of December 2025, DDS serves about 415,000 Lanterman‑eligible individuals and another 15,000 children ages zero through four who are provisionally eligible.
California Early Intervention Services Act Ensures Services for Eligible Infants and Toddlers. DDS also provides services via its Early Start program to any infant or toddler under the age of three with a qualifying developmental delay or who are at risk of developmental disability. There are no income‑related eligibility criteria. As of December 2025, DDS serves about 60,000 infants and toddlers in the Early Start program.
Regional Centers (RCs) Coordinate and Pay for Individuals’ Services. DDS contracts with 21 nonprofit RCs, which coordinate and pay for the direct services provided to “consumers” (the term used in statute). Services are delivered by a large network of private for‑profit and nonprofit providers. In addition to state General Fund and some smaller funding sources, these services are purchased in part through federal funding obtained through the Medicaid Home‑ and Community‑Based Services (HCBS) waiver. The HCBS waiver provides Medicaid funding for eligible individuals to receive services and supports in home‑ and community‑based settings, rather than in institutions.
Recent Rate Study Determines Payments for Services, Including Quality Component. For decades, the state paid DDS service providers according to an outdated and overly complicated rate structure that had not kept up with rising costs over time. In an attempt to modernize and rationalize this structure, the state commissioned a study of service provider costs that was completed in January 2020. The 2021‑22 budget began a multiyear, phased‑in implementation of a modernized rate model to pay service providers. The final stage of implementation has been in effect since January 1, 2025. Since this date, statute has required that the rates paid to service providers consist of two components: (1) a base rate equal to 90 percent of the rate model, and (2) a quality incentive payment equal to 10 percent of the rate model.
Most Services Provided to Consumers Enrolled in Medi‑Cal Receive Federal Funding. DDS can draw down federal Medicaid funding to support services provided to consumers who are enrolled in Medi‑Cal. For eligible services, costs are shared evenly between the federal government and the state. Nearly all home‑ and community‑based services coordinated by RCs are eligible to receive federal Medicaid matching funds. Such services include residential services, independent and supported living services, day programs, transportation, supported employment, and respite services. In addition, some of the time spent on case management by RC staff for consumers enrolled in Medi‑Cal is eligible for federal Medicaid funding. The department estimates that about 70 percent of consumers are currently enrolled in Medi‑Cal.
Recent Federal Legislation Makes Changes to Medicaid Eligibility but Exempts Those With Intellectual and Developmental Disabilities. In July 2025, Congress passed and the President signed H.R. 1, titled the One Big Beautiful Bill Act. Among other provisions, H.R. 1 imposes additional eligibility requirements for certain childless adults enrolled in Medicaid. H.R. 1 exempts some groups from these new requirements, including individuals with an intellectual or developmental disability and family caregivers of disabled individuals.
2026‑27 Budget Proposal
Overview
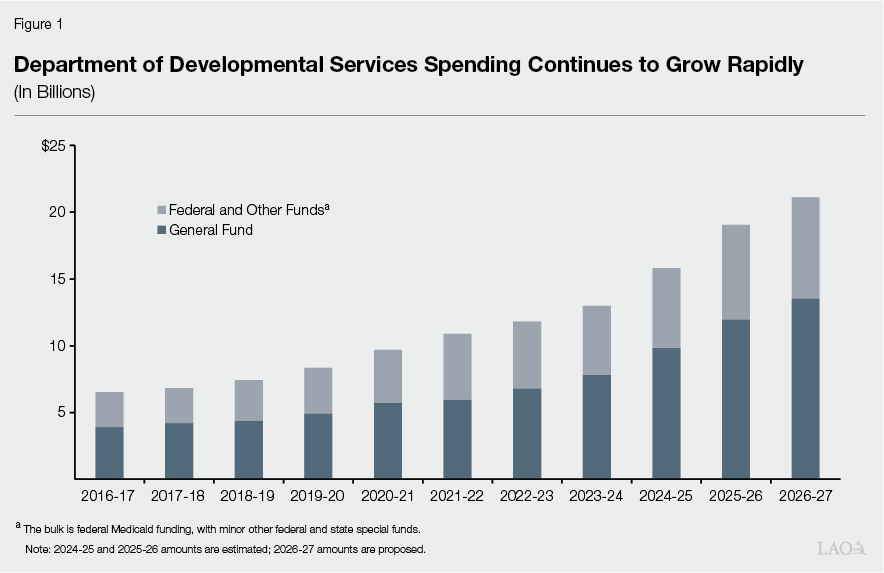
Proposed Budget Reflects Significant Growth. The Governor’s budget proposal includes $21.1 billion total funds in 2026‑27, up $2.4 billion (12.6 percent) over the revised 2025‑26 level ($18.7 billion). Of the proposed 2026‑27 total, $13.5 billion is from the General Fund, up $1.5 billion (13 percent) over the revised 2025‑26 level ($12 billion General Fund). Significant year‑over‑year growth in DDS spending is a feature of DDS budgets over the past ten years, as shown in Figure 1. We describe some of the main drivers of recent expenditure growth in DDS later in the report.
The administration projects that it will serve about 525,000 individuals in 2026‑27, up about 35,000 individuals compared to 2025‑26. This caseload projection is consistent with recent trends. We describe some of the factors that contribute to DDS caseload growth later in the report.
New Spending Proposals Are Small in Number and Total Cost. The Governor’s budget includes two discretionary spending proposals for 2026‑27. The first proposal would provide $5.7 million limited‑term General Fund to continue planning of an IT project first introduced in 2021‑22; the second proposal would provide $2.1 million General Fund ongoing to help the department comply with a recently finalized federal rule. We describe each proposal below and offer points for legislative consideration.
Proposed Funding to Continue Planning IT Project
DDS Planning IT Project to Replace Outdated Case Management, Accounting, and Reimbursement Systems. Since 2021‑22, the department has undertaken planning to modernize the IT systems used in the 21 RCs to support developmental services. RCs currently use separate and outdated IT systems for accounting and case management. The department also has a separate legacy system to claim reimbursements from the federal government. These systems date back to the 1980s, making them challenging and time‑consuming for department and RC staff to use. The case management systems are also inconsistent across RCs, as some RCs have adopted various “workarounds” over time to overcome shortcomings of the legacy system. Further, the existing systems do not allow consumers or their families to access their records electronically.
To address these issues, DDS is developing an IT project for a modern system that integrates accounting, reimbursement, and case management functions. The department envisions that the project, called LOIS (Life Outcomes Improvement System), will create consistency across RCs and allow consumers to view their own records electronically. DDS has completed the first two stages of the California Department of Technology’s (CDT’s) Project Approval Lifecycle (PAL) process, the state’s IT project approval process. We provide more detail on the history of the project, including previously appropriated funding, in last year’s analysis.
Department Conducted Additional Stakeholder Outreach on LOIS Project in 2025. DDS stated that, although it had previously conducted some discussions on desired outcomes for the project, these conversations did not adequately capture feedback from stakeholders. The department therefore undertook additional engagement in spring and summer 2025 with departmental staff, RC staff, providers, and individuals and families served. The department stated that feedback collected from RC staff and providers stressed the importance of streamlined processes, while feedback from individuals and families emphasized transparency and improved communication with RC staff. In fall 2025, the department consolidated this feedback into a set of seven themes that will guide the LOIS project moving forward. The themes include:
- Improving communication and collaboration.
- Supporting transparency and accountability.
- Centralizing information and education.
- Enhancing authorization and payment processes.
- Supporting person‑centered planning and outcomes.
- Improving system accountability and usability.
- Advancing consistency across RCs.
Project Received Limited‑Term Enhanced Federal Funding. In addition to $5.1 million General Fund allocated for IT project planning in 2025‑26, DDS also received enhanced funding from the federal government through the Advanced Planning Document (APD) process. DDS collaborated with the Department of Health Care Services (DHCS) to submit the required application materials to the federal government. The APD process allows the state to request a 90 percent match in federal funding (rather than California’s standard 50 percent match) to design, develop, and install IT systems that enable the state to more efficiently administer Medicaid benefits. DDS is eligible to receive this support because much of the project involves Medicaid‑funded services. This current round of enhanced federal funding is available to the department from June 2025 through September 2026.
Administration Requests One‑Time Funding to Continue Planning for LOIS in 2026‑27. The Governor’s budget proposes $5.7 million one‑time General Fund to continue the PAL process for LOIS. At the time of this report, DDS was working to complete Stage 2 of the PAL process, or the Alternatives Analysis. Stage 2 requires the department to conduct market research on which IT solution could meet the project’s desired outcomes, as well as develop a financial analysis for the recommended solution. The department released a Request for Information (RFI) in November 2025 with the goal of understanding industry best practices and vendor capacity for implementation. Responses to the RFI closed on January 23, 2026. The department stated that it aims to release a Request for Proposals (RFP) in 2026‑27 based upon the findings from the RFI. Additionally, DDS stated that it is working with DHCS to submit a renewed Planning Advanced Planning Document to continue enhanced federal funding beyond September 2026. Like the currently approved Planning Advanced Planning Document, this funding would similarly be limited term.
The department also proposed budget‑related legislation that would direct RCs to begin initial preparations for the transition to LOIS starting in 2026‑27. Specifically, the proposed legislation instructs RCs to prioritize data cleanup and limits RCs’ ability to adopt new IT systems or applications going forward (other than LOIS). The department stated that, although more time is still needed for planning and that a fully operational LOIS IT system is still a few years out, it intends to begin early preparations with RCs to make the eventual transition process smoother.
Reasonable to Continue Planning for LOIS, but Legislative Oversight Warranted. Given that the department has made progress in planning LOIS, it is generally reasonable to continue the PAL process, particularly in light of the administration’s success in securing enhanced federal funding. The continuation of the planning process for LOIS with the completion of the RFI and RFP processes will ultimately result in a cost estimate for the finalized IT project. (In an earlier and now outdated version of a planning document, DDS estimated that the project would cost about $135 million to $180 million in total funds, excluding future maintenance and operations costs.) The completed planning documents, including the cost estimate and projected time line to finish the project, will provide the Legislature with the information necessary to evaluate the merits of the proposed project. Given the fiscal constraints facing the state, legislative oversight of the LOIS project’s costs and progress will be particularly important. The Legislature could ask the department if, after the planning stage is complete, it intends to request enhanced federal funding for project maintenance and operations.
Proposed Funding to Implement Recent Federal Rule
The Governor’s budget proposes $2.1 million General Fund ongoing to implement the federal Home‑ and Community‑Based Services Access Rule, which was finalized in 2024. The requested funding will support nine permanent positions at DDS in 2026‑27 and ongoing. These positions had been approved for the same purpose on a limited‑term basis in 2025‑26. The final rule imposes a series of new requirements on states with staggered deadlines over the next several years. These requirements include establishing grievance systems for home‑ and community‑based services, reporting on service delivery timeliness, and establishing an advisory group on rates paid to direct care workers, among other items. According to the Centers for Medicare & Medicaid Services (CMS), the final rule is intended to increase transparency and accountability, standardize data and monitoring, and create opportunities for states to promote active beneficiary engagement. Given that CMS requires states to comply with the final rule, we consider this spending proposal to be nondiscretionary.
Oversight Issues
In recent years, the DDS system has undergone some significant changes as well as new initiatives that warrant continued legislative oversight. In addition, the DDS system faces a changing fiscal and policy landscape, including the implementation of H.R. 1 provisions affecting federal Medicaid eligibility and funding that warrants oversight. Given projected structural deficits, the Legislature will likely need to consider potential options for ongoing savings across the state budget. Understanding the cost drivers of DDS’ spending growth can help the Legislature better understand the fiscal dynamics of the program should solutions be needed. We discuss these oversight issues in the sections that follow.
H.R. 1 Implementation
Background
DDS Can Access Federal Funding Through Medi‑Cal. DDS can draw down federal Medicaid funding to support home‑ and community‑based services provided to consumers enrolled in Medi‑Cal. This federal HCBS funding has historically supported about 35 percent to 45 percent of total costs in DDS. Of the DDS consumers enrolled in Medi‑Cal, the majority (about 60 percent based on the most recent available data) qualify automatically because they receive Supplemental Security Income/State Supplementary Payment (SSI/SSP). A smaller share of consumers enrolled in Medi‑Cal qualify through the income‑eligibility pathway, including children whose families are income‑eligible. The LAO’s 2021 report, Enhancing Federal Financial Participation for Consumers Served by the Department of Developmental Services, provides more background on how Medicaid works in the DDS system.
Medi‑Cal Provides Health Care Coverage for Many DDS Consumers. Medi‑Cal is an important source of health care coverage for many DDS consumers, particularly those who lack commercial health insurance. For DDS consumers enrolled in Medi‑Cal, Medi‑Cal acts as the primary payer for their health care services. Under current law, the RC would generally become the payer of last resort for certain health care services if a consumer could demonstrate that no other source of coverage was available.
H.R. 1 Makes Changes to Medicaid Eligibility, but an Exemption Can Apply to DDS Consumers. H.R. 1 imposes new eligibility requirements on nondisabled childless adults who qualify for Medi‑Cal via their income (that is, excluding individuals who qualify automatically because they receive SSI/SSP). Specifically, H.R. 1 requires these adults to (1) verify that they have completed at least 80 hours per month of work, education, or community service, and (2) verify eligibility every six months, rather than every 12 months. Notably, H.R. 1 exempts certain groups from these new eligibility requirements, including individuals with an intellectual or developmental disability that significantly impairs their ability to perform one or more activities of daily living, as well as family caregivers of disabled individuals. This means that, as a matter of law, all DDS consumers enrolled in Medi‑Cal via the income eligibility pathway should be exempt from the new H.R. 1 requirements. The department stated that about 15,000 adult consumers are enrolled in Medi‑Cal via the income eligibility pathway.
Successful Exemption of DDS Consumers Depends on Administration’s H.R. 1 Implementation Plan. While the language of H.R. 1 indicates that states should exempt individuals with an intellectual or developmental disability and their family caregivers from new Medicaid eligibility requirements, the degree to which these exemptions are successfully implemented in California will depend on the administration’s approach. The administration, led by DHCS, has stated that it intends to maximize the use of existing data sources to confirm continuing eligibility of Medi‑Cal enrollees without burdening enrollees with paperwork. DDS indicated that it has already been working with DHCS to match information across each department’s records with the goal of automatically exempting all 15,000 adult DDS consumers in the income eligibility pathway from the new requirements. This could be more challenging for consumers’ family caregivers, as RCs maintain information on family caregivers for children, but less so for caregivers of adult consumers.
RC Staff Can Assist Consumers With Their Medi‑Cal Enrollment. While county governments manage all Medi‑Cal eligibility determinations, DDS consumers can request assistance from their RC in applying for and maintaining Medi‑Cal coverage. DDS indicated that it intends to collaborate with RCs to monitor any potentially emerging workload needs resulting from H.R. 1‑related requests for assistance from consumers.
Assessment and Issues for Legislative Consideration
Legislative Oversight Can Help Minimize Potential Adverse Impacts of H.R. 1. The Legislature will likely want to engage in oversight to ensure that DDS consumers in practice are exempt from the new H.R. 1 requirements to the maximum extent possible. Aside from potential disruptions to individual consumers in their access to health care coverage, any errors in the exemption system could also have broader fiscal implications for the state. This is because any loss in Medi‑Cal eligibility will reduce the amount of federal reimbursements that DDS can claim for RC‑coordinated services. Additionally, loss of Medi‑Cal coverage could require RCs to pay for health care services for consumers at full cost to the state if no other source of care is available. Continuing legislative oversight will help ensure that exemptions for DDS consumers are implemented as intended. Questions to ask the administration at budget hearings could include the following:
- Is there a role for RCs to educate individuals and families served on the upcoming changes from H.R 1.? If so, how would DDS oversee this effort?
- How will DDS collaborate with DHCS in the coming months to ensure its planned processes are successful in exempting all eligible DDS consumers from the H.R. 1 eligibility requirements? What is the role of the California Health and Human Services Agency in this process?
- It is possible that the state’s new automated data matching processes could fail to automatically exempt some DDS consumers from the H.R. 1 eligibility requirements. If this were to occur, what systems will be in place to identify these cases and notify the appropriate RC in a timely manner so that the RC can correct the error?
- The department stated that its budget projections for 2026‑27 do not incorporate any potential added costs due to the changes in H.R 1. Will the department be able to determine whether its costs increase in the future due to H.R. 1? If so, how?
Update on Service Provider Rate Reform and the Quality Incentive Program
Background
Service Provider Rate Reform Intended to Improve Access to Services. The state initiated a rate study for DDS services in part because the historical rate structure did not result in funding levels for service providers that kept pace with system growth or supported an adequate supply of providers. The funding to implement the rate study’s recommended rate models was phased in beginning in 2021‑22, ramping up to current levels by 2024‑25. The increased funding was intended to support a sufficient supply of quality service providers by raising funding levels for providers via increased rates. We provide more background on rate reform in our 2024 report, The 2024‑25 Budget: Department of Developmental Services.
Rate Reform Also Focused on Quality of Services and Outcomes. State statute (Chapter 76 of 2021 [AB 136, Committee on Budget]) establishes legislative intent that rate reform implementation should help the developmental services system focus on outcomes. To achieve this, statute specifies that provider payments should be linked to consumer outcomes. Specifically, statute provides that the fully funded provider rate models are to be implemented using two payment components: a base rate equaling 90 percent of the rate model and a quality incentive payment equaling up to 10 percent of the rate model, the latter of which is to be implemented through the quality incentive program. Statute also establishes that performance metrics should evolve from initially being more process‑related (such as providers completing certain tasks by set deadlines) to eventually include outcome measures (such as whether individual consumers are able to achieve their goals). The goals of individual consumers can vary widely and span from short to long term. Such goals could include living in an apartment, getting and maintaining a job, and participating in music or art classes.
Quality Incentive Payments in Place Since 2025. The final phase of rate reform has been implemented since January 2025. Since this time, rate models are fully funded, with the 90 percent (base rate) and 10 percent (quality incentive payment) structure set out in statute. For the period spanning from January 1, 2025 through June 30, 2026, providers could earn the quality incentive portion of rate models by enrolling in DDS’s Provider Directory.
As a budget solution, the 2025‑26 Budget Act added three criteria that providers must satisfy to be eligible to earn a quality payment equal to 10 percent of the rate model beginning in July 2026 (in addition, providers would still need to meet quality benchmarks to earn the additional payment, as described next). Specifically, in order to be eligible, providers must (1) comply with Electronic Visit Verification, (2) comply with the federal HCBS Settings Rule, and (3) complete independent audits or reviews if total payments from RCs are above a certain threshold. Providers must satisfy these requirements by February 27, 2026 to be eligible to receive a full fiscal year of quality payments for 2026‑27. Stakeholders have recently expressed concerns about the challenges of meeting this deadline for independent audits and reviews, particularly for providers at or near the payment threshold. In response, the department released guidance on February 11, 2026 indicating that providers will have the opportunity to earn a partial year of quality payments if they come into compliance after the February 27 deadline.
For the period spanning from July 1, 2026 through June 30, 2027, providers can earn the quality incentive portion of the rate models by completing surveys about workforce capacity and service delivery. (Providers must complete the surveys in addition to satisfying the three criteria listed in the previous paragraph. The deadline for providers to complete the surveys was February 27, 2026.) To encourage survey completion, the department offered trainings to providers on the data collection surveys and sent weekly e‑mail reminders to remind providers to submit their data before the deadline.
Department Collecting Data to Inform Future Quality Metrics. The department stated that the provider surveys will form a baseline for the development of future quality measures. Specifically, the department is collecting data about providers’ workforce capacity (staffing, vacancies, wages, and turnover), service delivery (where, how, and in what languages services are provided), and data specific to providers of employment services and providers of residential services. By measuring these existing practices, the department intends to have a better sense of average performance across providers. This will help the department determine the levels of performance that would be reasonable as a standard for future quality measures. The department indicated that early attention to these process‑oriented measures will help prepare for eventually measuring individual outcomes. Per statute, any metrics or benchmarks for individual outcomes must be established with input from stakeholders through public meetings and 30‑day public comment periods. As part of this, the department has convened a Quality Incentive Program workgroup since 2021, which has helped to select previous quality metrics.
Assessment and Issues for Legislative Consideration
Will Department Need to Update Its Estimated Savings Compared to June 2025? In June 2025 at budget enactment, the department estimated that it would save $222 million in ongoing General Fund savings by imposing the three additional “pre‑qualifiers” that providers must satisfy in order to be eligible to earn a quality incentive payment. The actual savings achieved from this budget solution in 2025‑26 will depend on the number of providers who fail to comply with the new requirements. Given the department’s recent decision to allow providers to earn a partial‑year payment if they miss the initial deadline, it is possible that savings will erode from the original estimate. The Legislature could ask the department at budget hearings to provide an updated savings estimate for this budget solution.
How Will the Quality Incentive Program Balance Meaningful Standards With Achievability? The department indicated that future quality metrics will be based upon a benchmark of providers’ current performance. As future quality metrics are established, the department will need to work with stakeholders to determine its definition of “quality” services and individual outcomes. In practice, quality can be challenging to measure given the expansive nature of an individual’s well‑being and the many outcomes involved. Future metrics should be sufficiently robust to reinforce quality, but not so stringent that a large share of providers fail to meet the standards across multiple years and potentially risk ongoing revenue losses due to reduced payments. The department has stated that it intends to approach the quality incentive program as an iterative process. Future iterations could provide opportunities for legislative engagement and oversight.
Will Providers That Fail to Satisfy Future Quality Measures Receive Technical Assistance to Improve Performance Going Forward? Providers have expressed concerns about whether the department or RCs will offer technical assistance to providers that fail to meet quality measures in a given year. The department has stated that its goal is to have as many providers as possible earn the quality payments, but it has not yet discussed how it might approach circumstances in which providers do not achieve them. The Legislature could ask the department at budget hearings to share its current thinking on whether it is contemplating providing technical assistance to support providers, and if so, how such effort could be funded.
Cost Drivers in DDS
Given Projected Structural Deficits, Better Understanding of Spending Growth Drivers Important. In light of projected structural budget deficits, we recommend that the Legislature closely examine General Fund spending across the budget, including in DDS. We provide this information to help inform the Legislature’s deliberations and conversations about its budget priorities over the coming months and years. This section identifies the major drivers of spending in DDS. Where relevant, this section notes where there are potential levers available if the Legislature wishes to adjust spending. The Legislature could have greater insight into these spending drivers, as well as potential spending adjustments, if the department were to provide richer data.
Four Key Factors Drive Spending in DDS. As discussed in the analysis that follows, the Lanterman Act, due to its foundational role, influences all cost drivers in the developmental services system. These cost drivers (similar to other health and human services programs) include caseload, available services, utilization of services, and the rates paid for services. Assuming that the Lanterman Act continues to serve as the foundational policy for the state’s developmental services system, the Legislature generally has relatively limited discretion to control spending growth by adjusting caseload or utilization. The Legislature has previously suspended access to certain services in times of budget challenges, but this choice raised equity concerns among stakeholders and was only temporary. While the Legislature does have some discretion over rates, any significant reductions in this area would likely give rise to policy trade‑offs, such as reducing consumers’ access to services for which they are eligible. The following paragraphs describe each of the main cost drivers in more detail after first discussing the role of the Lanterman Act in influencing these cost levers.
The Role of the Lanterman Act
The Lanterman Act Is the Foundation of California’s Developmental Services System. The Lanterman Act has served as the foundational policy of the DDS system and has long guided legislative decision‑making. The act outlines duties for DDS and establishes that the state “accepts a responsibility for persons with developmental disabilities and an obligation to them which it must discharge.” It also gives people with developmental disabilities the right to receive services and supports to help achieve their goals. Our analysis in this section assumes that the Lanterman Act remains in place as reflected in current law.
The Lanterman Act’s Statutory Entitlement Sets California Apart From Other States. As mentioned earlier, the Lanterman Act amounts to a statutory entitlement to services and supports to individuals with a qualifying disability (broadly defined). Unlike other states, California does not impose a cap on the number of individuals that can be served through DDS and therefore does not maintain a waitlist for individuals to be evaluated and become eligible to receive services. Additionally, California does not require that individuals need an institutional level of care to receive services, whereas some other states maintain such a requirement. Further, unlike other states, the Lanterman Act does not impose any time limits on eligibility.
The Lanterman Act Grants Access to Services According to Each Consumer’s Choices. The Lanterman Act guides the availability and delivery of services in DDS. The act states: “An array of services and supports should be established which is sufficiently complete to meet the needs and choices of each person with developmental disabilities, regardless of age or degree of disability, and at each stage of life and to support their integration into the mainstream life of the community.” In this way, the act allows for variety in the range of services available to DDS consumers. The act also states that these services should enable people with intellectual and developmental disabilities to have the same patterns of living as people without these conditions, and that consumers should be empowered to participate in decisions about their services.
Data Limitations
While the department provides some data on spending drivers, publicly available data are fairly limited. This means that the Legislature’s ability to understand spending drivers at a more nuanced level is limited. While the department publishes caseload and service expenditure data on a regular basis, these data are generally presented on an aggregate basis. Importantly, the department does not currently publish detailed data on the utilization of services. For example, the department’s budget documents note that changes in service expenditures in the budget year are due to changes in utilization, but do not provide information to understand the nature, extent, and drivers of these changes in utilization. Accordingly, data are not readily available to be able to know how many consumers are using a particular service and at what intensity the service is being used. The following analyses largely rely upon publicly available data, with some additional data provided by the department upon request.
Caseload
DDS Caseload Determined by Number of Individuals Identified as Eligible for the Lanterman Act’s Entitlement. The Lanterman Act requires DDS to serve all individuals determined eligible by an RC. The program has never required means testing, so income is not considered when an individual applies for services. The department also does not limit eligibility based on immigration status and does not collect information on consumers’ immigration status. Compared to other health and human services programs such as Medi‑Cal, there is little “churn” in the system, or individuals cycling in and out over time. Most DDS consumers are served by the system for their entire lifespan once they are deemed eligible. RCs are responsible for providing assessments and diagnoses to determine eligibility; this process can include a review of an applicant’s records as well as tests performed by doctors and/or psychologists. RCs can contact family members, doctors, schools, or other state agencies to request information relevant to the eligibility determination (with the applicant’s consent). If an RC determines that an applicant is not eligible for services, the applicant can appeal the decision.
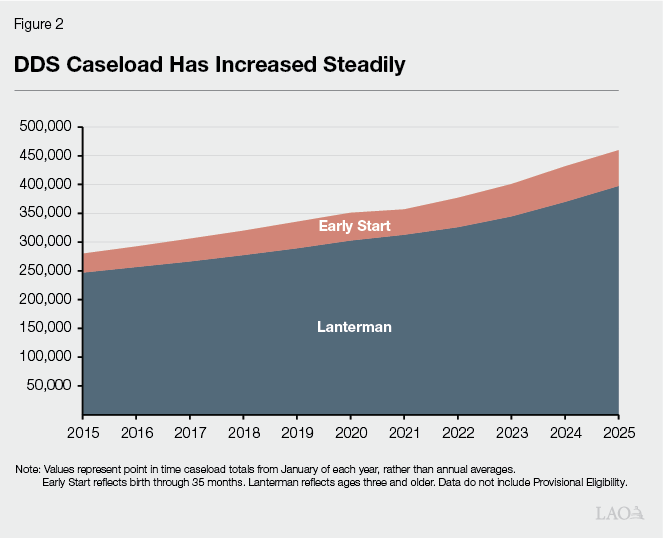
Caseload Has Steadily Increased Over Time, Driven Mainly by Diagnostic Changes and Increased Outreach. As Figure 2 shows, DDS caseload has increased notably over the last ten years, with an average annual growth rate of about 5 percent in total caseload from 2015 through 2025. This is faster than the population growth in the state over this period. Caseload increases are driven by the diagnosis of qualifying intellectual and developmental disabilities among California residents. The National Center for Health Statistics found that the prevalence of any diagnosed developmental disability in children aged 3‑17 years in the United States increased by about a full percentage point (from 7.40 percent to 8.56 percent) between 2019 and 2021—a significant change in a short period of time. From 2015 to 2024, California’s population of minors whose families self‑report a cognitive or self‑care disability grew at an annual rate of about 4 percent. One key caveat is that these estimates do not necessarily correspond to official diagnoses of any particular condition.
In recent years, the department has noted an increase in the share of consumers diagnosed with autism, while diagnoses of intellectual disability have decreased. The share of consumers diagnosed with autism increased from about 30 percent in 2016‑17 to about 40 percent in 2024‑25. This trend is not unique to California. Research suggests this trend could partly reflect more awareness and outreach among previously underserved communities, as well as evolving approaches to diagnosis and evaluation.
Caseload increases are also partially driven by outreach and education to those potentially eligible. Early Start’s caseload of infants and toddlers has also recently increased, likely in part due to better identification of eligible families. For example, Medi‑Cal has increased access to diagnostic screenings over time. Additionally, DDS stated that it has increased outreach efforts to identify babies and toddlers potentially eligible for Early Start services since the COVID‑19 pandemic. The department expanded these outreach efforts so that more children, as well as their families, could receive supportive services earlier in life. (A review of academic literature on early intervention suggests that these programs have a positive effect on developmental progress for participating children.) Early Start caseload experienced an average annual growth rate of about 6.5 percent from 2015 through 2025.
Finally, the adult caseload is also affected by the trend that lifespans for people with intellectual and developmental disabilities have generally increased over time due to improved access to services and supports. This means that more individuals are staying in the system for longer.
Caseload Is a Key Contributor to Spending Growth. Total caseload (of Early Start and Lanterman caseload, excluding presumptive eligibility) has increased from about 280,000 individuals served in 2015 to about 460,000 individuals served in 2025. This represents about a 60 percent increase. Once a person is deemed eligible to receive services through their RC, the Lanterman Act provides that they are entitled to receive the services they need for their entire lifespan. This arrangement means that, as caseload increases, costs also increase.
Services
DDS Budget Largely Dedicated to Purchasing a Variety of Services. Most of the DDS budget (about 90 percent of total funds in 2025‑26) is spent on the purchase of services for consumers. DDS allocates funding to the RCs that determine which services each consumer will receive and purchase these services on behalf of consumers. The types of services that consumers can receive through their RC include behavioral services, day programs, employment supports, medical care, residential services, respite (providing breaks for family caregivers), social recreation, support and training, and transportation. The DDS budget only accounts for services purchased by RCs; it does not reflect services paid for by other sources (such as CalFresh, In‑Home Supportive Services, or county services). As Figure 3 shows, spending on services purchased for consumers has more than doubled across all service types. Importantly, the increased cost for services also reflects a combination of the increases in caseload and utilization over time.
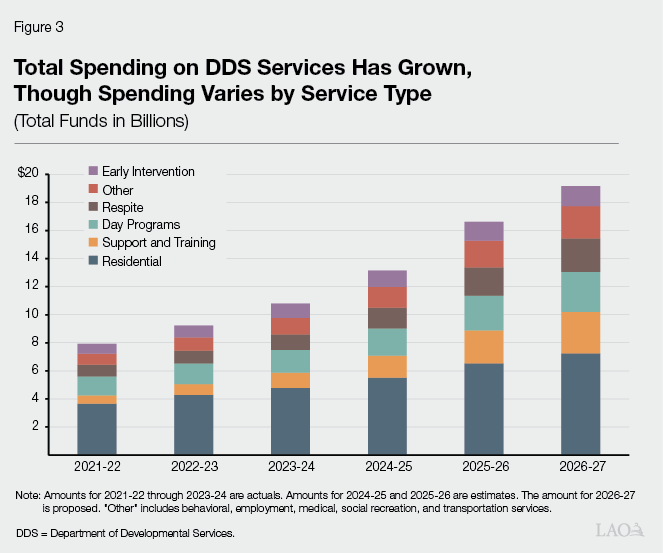
Individual Services Vary in Growth Rates and the Relative Share of Expenditures Over Time. Across all services, the average annual growth rate in spending from 2021‑22 to 2026‑27 (proposed) is 19 percent. There is significant variability in the average annual growth rate by individual service (many individual services are captured in “Other” in the figure), ranging from a low of 3 percent (employment services) to a high of 52 percent (social recreation). Residential, day programs, and early intervention services have average annual growth rates below or equal to 19 percent, while respite and support and training services have average annual growth rates above 19 percent. Additionally, there has been some change in the relative contribution of each individual service to total services spending over the 2021‑22 to 2026‑27 period. For example, the spending share of residential services has decreased from 46 percent to 38 percent, while the spending share of support and training services has increased from 8 percent to 15 percent.
Costs Vary by Type of Service, With Delivery Models Evolving Over Time to Emphasize Individualized Supports. The Lanterman Act specifies that services overall should be provided in a cost‑effective way. Certain services cost more per unit than others depending on the comprehensiveness of the service and the way it is delivered. For example, some services must be provided by licensed professionals and therefore have higher rates. Residential services, which include independent and supported living services either in a consumer’s home or in licensed facilities that provide 24‑hour nonmedical residential care, typically have a relatively higher cost per person due to the comprehensiveness of the service provided (including personal services, supervision, and/or assistance essential for self‑protection or completing the activities of daily living). Some licensed facilities are tiered based on the level of services offered, with higher tiers typically coming at a higher cost because the services require more staff hours per week. This arrangement ensures that consumers with relatively higher support needs can receive professionally supervised services in an appropriate setting.
Additionally, certain services can be provided in a group setting at a lower cost per person, whereas other services are provided individually at a higher cost per person. Over time, best practices in developmental services have evolved to place a greater emphasis on individualized services. This can result in higher costs, both because there are fewer group settings and because services are more tailored to each consumer. Recent federal rules reinforce this growing emphasis on a more personalized approach to services. Specifically, these rules require that individuals receive services in the most integrated setting and emphasize a person‑centered approach to service planning.
Utilization
RCs Develop Individual Program Plans (IPPs) to Determine Utilization of Services. The Lanterman Act tasks RCs with developing an IPP for each consumer, a document that outlines the services that a consumer will receive and in what amount to meet their stated goals. It is intended that the IPP reflect each individual’s needs and preferences. Service coordinators at RCs follow the RC’s purchase of service policies, which must be approved by DDS, to determine which services are appropriate to help a person meet their goals in accordance with the Lanterman Act. In this way, RCs act as utilization managers through the application of purchase‑of‑service policies. After the initial IPP meeting, RCs are required to meet with each consumer to review their IPP at least once per year. RCs must obtain a consumer’s agreement to the IPP. If a consumer disagrees with their RC’s decision to change, reduce, or stop a service in the IPP, the consumer can appeal the decision.
Individual Utilization Varies Widely According to Consumers’ Needs. As data are not readily available on the number of consumers that utilize each of the wide variety of services available through the RC system, it is not possible to assess trends in the utilization of given services over time. While data showing the number of consumers using a particular service would allow for better analysis of trends, even richer data for analysis would include the intensity of service utilization at the individual consumer level. This is because individual utilization within each service category can vary widely based on each consumer’s needs as identified in the IPP. For example, one consumer might receive five hours of respite in a given month, while another consumer might receive 20 hours of respite in the same month. Accordingly, using available data to calculate an average cost per consumer ($21,000 General Fund in 2025‑26, for example) or a growth rate in the average cost per consumer (8.6 percent between 2021‑22 and 2026‑27, for example) masks a wide range of variation in expenditures per consumer across the entire population served.
In addition to variation across consumers, utilization can also vary throughout an individual consumer’s lifetime. For example, between the ages of three and 22, consumers receive services primarily through their local school district rather than their RC. During this time, utilization of services purchased by the RC is low. After age 22, utilization of RC‑purchased services will increase for most consumers. Any analysis of utilization would also require information on consumers’ ages to account for these differences. As another example, a consumer’s utilization of services would likely change if their goals change (such as deciding to move out of the family home and into a separate residence, or deciding to request employment supports to obtain a job). The annual IPP meetings are intended to capture such changes and adjust services accordingly.
Service Utilization Also Impacted by Availability of Providers. Under the Lanterman Act, RCs are responsible for connecting consumers to provider organizations that can provide the services agreed upon in the IPP. In some cases, even if the RC authorizes a service, a provider might not be immediately available to fulfill the need. This could be for several reasons (for example, local providers are already at capacity with existing clients, or there are no local providers that speak the consumer’s language). In such cases, the consumer would likely need to wait until a provider is available before they can receive the authorized service. Actual utilization can therefore be lower than authorized utilization. RCs publish annual reports on the share of authorized services that were actually utilized, but the reporting is not consolidated across RCs statewide. Additionally, the annual reports do not break out total authorization or utilization by service type.
Legislature Has Recently Focused on Increasing Access to Services. Over the past several years, the Legislature has taken actions intended to mitigate barriers to service access and utilization. In 2016, the Legislature appropriated ongoing funding for the Disparity Funds Program, which awards grants to RCs and community‑based organizations for strategies to reduce disparities in service authorizations, utilization, and spending. Since 2021‑22, the Legislature has also authorized funding for programs intended to strengthen and stabilize the provider workforce in order to establish a more reliable provider network and improve access to services. In 2023, the Legislature codified several efforts to make processes across RCs more consistent in order to improve access to services statewide (Chapter 192 of 2023 [SB 138, Committee on Budget and Fiscal Review]). These efforts include establishing common data definitions to promote service access and equity in all RC services, creating a standardized IPP template, establishing standardized procedures for providers to contract with RCs, and developing recommendations to address inconsistencies in the availability of services or supports across the state.
Rates
State Recently Overhauled Service Provider Rates, With Goal of Improving Consumer Outcomes. As discussed earlier, the state began implementing rate reform in 2021‑22, with the goal of supporting a sufficient supply of quality service providers and improving consumer outcomes. Now that rate reform is fully implemented, the administration estimates that the annual cost is about $3.5 billion total funds ($2.1 billion General Fund).
State Minimum Wage Also Increases Rates. In addition to rate increases implemented under service provider rate reform, the statewide minimum wage also increases DDS rates. Rate models for DDS services are automatically increased whenever the state minimum wage increases. Chapter 4 of 2016 (SB 3, Leno) has gradually increased California’s statewide minimum wage from $8 per hour to $16 per hour. Under SB 3, the statewide minimum wage will continue to increase by up to 3.5 percent each year, depending on inflation. In recent years, the cumulative cost of annual minimum wage increases under SB 3 have represented about 5 percent to 10 percent of General Fund spending on services purchased for DDS consumers.
Legislature Has Some Discretion Over Rates, But Faces Trade‑Offs With Service Access Impacts. Given that the rate increases adopted under rate reform are intended to increase access to services, the Legislature would likely want to consider whether any potential reductions to rates could reduce access. Additionally, because many DDS services receive federal Medicaid matching funds for eligible consumers, these services are subject to Medicaid rules. A recent federal rule in Medicaid now requires states to demonstrate that any proposed changes to provider rates will not negatively impact individuals’ access to Medicaid‑funded services. If the Legislature wanted to consider savings in DDS rates, it could request collaboration with the department (and the department’s third‑party consultant that developed the current rate models) to carefully consider whether there are any rates that could be adjusted without significantly reducing access to services.
Issues for Legislative Consideration
Legislature Requires Richer Data to Consider Cost Drivers and Spending Adjustments. Moving forward, the Legislature may wish to better understand program dynamics in DDS, both in terms of fiscal considerations as well as service levels provided to consumers. The data that are currently publicly available provide some insight into these questions, but do not provide a holistic picture of the DDS system. Without ready access to richer service utilization data detailing consumers’ service level and cost, the Legislature can only draw narrow or incomplete conclusions about trends in the program. In addition, the Legislature is hampered in its ability to fully assess the programmatic impacts and trade‑offs of proposed spending adjustments (both spending proposals and budget solutions). Lacking robust data on DDS program dynamics, the state in previous periods of budget challenges often enacted budget solutions that were blunt and not targeted well to minimize adverse programmatic impacts. Such solutions included across‑the‑board provider rate reductions and the full suspension of a particular service. Going forward, richer data could help the Legislature take a more targeted approach to minimize programmatic harm, retain services to the extent possible to consumers with the highest needs, and reduce the potential for increasing disparities among consumers.
Legislature Could Work With Administration on Revised Data Reporting. The Legislature could consider collaborating with the department to determine the nature and content of a more robust public data reporting requirement placed on the department. This reporting requirement should consider the feasibility of data collection and the usefulness of the data for legislative analysis. Data should help the Legislature be more informed when working with the administration on spending adjustments going forward. It is also important to note that the recently created Provider Directory, as well as the proposed LOIS project, could facilitate this type of reporting. The Legislature could ask the department about how its planning for the Provider Directory and LOIS could accommodate statewide data collection and reporting.